Learning Objectives
This is an intermediate-level course. Upon completing this course, mental health professionals will be able to:
- Discuss the interaction between personality and temperament.
- Describe research findings regarding environmental and biological influences on anorexia nervosa.
- Explain why Temperament Based Therapy with Support (TBT-S) advocates the inclusion of supports in adult eating disorder treatment.
- Discuss the evidence for the role of anxiety in anorexia nervosa.
- Provide two TBT-S strategies for addressing altered decision-making and inhibitory control in anorexia nervosa.
This course introduces treatment providers to a new treatment approach that augments their current eating disorder treatment by filling in the biological bases of the illness and applies brain-based responses to treatment applications. As neurobiological research continues to emerge, and international research findings on TBT-S increase, treatment significance will continue to be refined. Risks could occur if clinicians present the research findings as absolute instead of comparing neurobiological findings with their clients’ experiences for the clients to better clarify what they are experiencing in their illness and why.
Outline
- Introduction
- What Is Temperament Based Therapy with Support (TBT-S)?
- Why TBT-S Began by Focusing on Anorexia Nervosa
- TBT-S Description
- What Is Temperament, and Why Is It Important?
- Who Are the Intended Participants?
- Where Can TBT-S Be Applied?
- TBT-S Modular Structure
- Two TBT-S Versions:
Young Adult (YA) and Severe-and-Enduring Anorexia Nervosa (SE-AN)
- TBT-S Core Principles
- Eating Disorders Are Brain- and Biologically Based Disorders
- Treat to the Trait: Targeting Temperament in Treatment
- Food Is Medicine
- Supports Are a Necessary Part of Treatment
- Movement and/or Actions Are Fundamental to Change
- Overview of Selected Intervention Strategies
- How to Deliver Neurobiology Psychoeducation as a Motivational Strategy
- Who Is Involved
- What Is Needed
- Content
- What Does the Research Say?
- Psychoeducation Module Instructions
- TBT-S Neurobiology Psychoeducation Module: Anxiety and Interoception
- When Is This Module Provided?
- Who Is Involved
- What Is Needed
- Content
- TBT-S Neurobiology Psychoeducation Module: Decision-Making and Inhibitory Control
- Objective
- When Is This Module Provided?
- Who Is Involved
- What Is Needed
- Content
- Nondominant Hand:
TBT-S Neurobiological and Problem-Solving Experiential Activity
- Neurobiological and Trait Targets
- Objectives
- Who Is Involved
- Materials and Time Needed
- What Does the Research Say?
- Clinician Checklist
- Experiential Activity Instructions
- Rule
- Steps and Scripts
- How to Treat to These Traits
- Homework
- Conclusion
- References
Introduction
This course addresses a novel treatment approach for Eating
Disorders, Temperament Based Therapy with Support, aka TBT-S. TBT-S has
initially focused on eating disorders due to the high mortality rate and the
lack of effective treatment over time. Yet TBT-S holds the potential to be
studied and applied to all mental disorders that are trait based, such as
anxiety or obsessive compulsive disorder.
This course is based on the book, Temperament Based Therapy with Support for Anorexia Nervosa:
A Novel Treatment, by Hill, Peck and Wierenga (2022, Cambridge University
Press, England).
TBT-S is a treatment of doing. This course is as much about
“trying on” neurobiological ideas and concepts as it is about reading about
them. It introduces the reader to
what this new treatment is and provides examples of TBT-S treatment tools and skills for clinicians, dietitians,
medical professionals, and educators, and how it could be applied in various types of therapeutic and educational settings.
Eating disorders are one of the most misunderstood and yet deadly
of all mental disorders. The diagnostic name, “Eating Disorder” (ED) reflects
the little that was known when initially described in the DSM-III[1] in
1980. Treatments then and now focus primarily on symptoms, outward problematic
expressions of thoughts, feelings, and behaviors.
However, eating is a requirement of life, not a disorder.
Everyone eats, but not everyone has an eating disorder. The diagnostic name set
the stage for people to either downplay an everyday requirement of life or
distance themselves from the poorly understood illness. Misunderstanding of EDs
became targeted against adolescent white girls who were described as being on a
campaign to over-control their appearance. Social, cultural, family, and
analytic theories abounded addressing outward symptoms. What was missing? The
underlying biological causes of the illness, i.e. the genetic, neurobiological,
and temperament bases.
It was not until after the genome was sequenced in 2000 and
technology became more refined in the early 2000s that researchers could begin
to look inside the brain in a 3-D functional way while activities were being studied,
in order to observe brain response. Walter Kaye, at UCSD, led this research
globally. His groundbreaking article in 2009 that identified brain circuits
that fire significantly differently between those who had eating disorders and
those who did not, indicated that there was much more going on in brain
response than ever imagined. The last 20 years of research has continued to
refine what is happening on the inside of the brain of those with EDs, while
also identifying genetic differences and temperaments that set up ED
vulnerability.
Temperament Based Therapy with Support, TBT-S,
emerged out of the growing biological eating disorder research. It describes Eating
Disorders as grounded in traits, which are genetically caused and
neurobiologically defended. From the moment of conception, the genetic makeup
of the ovum becomes the recipe for the brain to begin wiring to express
inherited traits. This wiring is both biological, such as height, and temperament
based, such as extroverted.
One’s temperament is the biological/“nature” side of personality
and consists of traits. Character is the social or “nurture” side of
personality. While the research community’s main population distanced
themselves from being associated with eating disorders, clinicians have tended
to distance themselves from genetic and neurobiologically based research into what
has more recently been found to be the very nature of the illness. Many
graduate programs still do not offer neurobiological mental health courses.
This results in a huge gap in clinician understanding of EDs and perpetuates
the sole use of past theories and symptom-focused therapies. The mental health
world has remained flat, when in fact it is 3-D and round.
TBT-S is a treatment that integrates genetic, neurobiological,
and temperament research into treatment applications to augment ongoing
therapies. The TBT-S approach provides clinicians with a framework to apply other therapies. It provides the
biological bases of the illness that offer direction signs for what
intervention to apply and when.
If symptoms are the limbs of a tree, then traits are the roots. An
evergreen tree can never be a deciduous tree, nor should it. There are many
variations of any one type of tree, such as variations of oak or variations of
spruce. Yet, mental health providers are often trained to approach clients with
the same therapeutic expectations in spite of widely diverse traits. A person’s
traits, drawn from their temperament, do not go away. While we work to reduce
or eliminate symptoms, a person’s traits are with them for life. However,
clinicians are often not taught the difference between symptoms and traits and
may erroneously work with clients to eliminate their traits, or aspects of who
they are, such as being impulsive, rather than working on their symptoms. This sets the
client up to fail, lowers motivation, and increases treatment dropout.
TBT-S works with clients to identify their traits and use them as
strengths. Traits are traditionally taught and viewed as pathological. TBT-S
provides clinicians with a means to identify clients’ temperaments, and methods
on how to reshape clients’ destructively expressed traits to be more
productively expressed over time. For example, while an impulsive trait cannot
be eliminated, shifting the impulsivity from destructive binges to impulsive
writing and research “binges,” as one client did, can result in clients
becoming a better version of themselves.
Scripts are in italics throughout the course. Clinicians are
encouraged not to read the scripts verbatim but instead to learn the points and
share them in their own voices.
The treatment name, Temperament Based Therapy with Support, uses the
word “Support.” Adult clients with anorexia nervosa chose this word themselves.
They shared that they did not want people to whom they turned for support to be
labeled as “caregivers,” because they did not want to be “taken care of.” Adult
clients requested that they be referred to as “Supports.” In many cases, these support
persons extend far beyond their parents and family of origin. “Family” in family-based
therapy is descriptive for adolescents with an eating disorder (ED). Adults with
ED, however, reported they preferred a broader descriptor for people to whom they
turn for support. They chose the word “Supports” to describe both the people
and the actions they need from them. The word in the treatment title, Support, becomes
a two-for-one term. “Supports” is capitalized throughout the course, referring to
the persons to whom adult clients turn for support.
Regarding diversity, this course addresses the underlying biological
aspects of eating disorders. Fundamentally and metaphorically, every race and
culture has the same biological color. It is red, the color of blood. Basically,
everyone has the same organs, blood types, bones, and brain structures
regardless of culture or race. Skin color is a result of genetic inheritance
and unto itself does not biologically contribute to eating disorders.
Environmental and cultural influences shape inherited traits. If
a person of any race or culture inherits traits that are proving to increase
vulnerability in developing an eating disorder, then that person may develop
the illness, regardless of race or culture. Gender does impact Eating
Disorders due to biological causes. Eating disorders are primarily a female
illness due to biological, specifically hormonal/gonadal, responses
interplaying with temperament. Our open trials included persons across the
gender continuum.
In addition, persons who experience trauma and have traits that
are vulnerable to eating disorder development, may develop an eating disorder
after experiencing the trauma. The trauma appears to be the trigger that
intensifies the person’s traits to become more extremely expressed, but the
trauma is not the sole cause of the illness. As discussed in the book, while
social pressures to be thin may vary across cultures, genetic researchers have
found that social pressures are secondary to genetically triggered traits from
adolescence through older adulthood. Genes override environment from one’s
teens throughout life as is described in the sections below. It is how the inherited
traits are shaped that matters. Environment, therapy, families, friends, and
communities hold that role.
Each section that follows provides “bite-size” chunks of information concisely
describing what practitioners and educators who have little neurobiological training
or knowledge can learn and use to share with their clients or students. Each
section is a module that could be offered in any one session or classroom, and integrated
into ongoing therapy sessions or classroom lectures. Each section has bottom-line
points that if nothing else is remembered, are “key points” for the reader to hold
onto and use.
Just as the structural foundation of a house is critical in
providing a firm and solid foundation for the rooms built upon it, so too is
the research that grounds this treatment. TBT-S is grounded in research.
Research is the vital component that creates the walls and structural bases of
the treatment. That is why the references are provided. The reader is referred
to references that repeatedly explored more deeply the genetic, neurobiological,
and temperament factors of eating disorders that grounds TBT-S. We urge you to
refer to the references for more depth.
What Is Temperament Based Therapy with Support (TBT-S)?
Why TBT-S Began by Focusing on Anorexia
Nervosa
Anorexia nervosa (AN) is a serious, life-threatening condition that
has one of the highest death rates of all mental illnesses.[1–4] It is
diagnostically defined as having extremely low body weight, an intense
fear of weight gain, and disturbance in how one’s body weight and shape are
experienced.[5] It occurs primarily in females,[6] usually
taking form during puberty with the potential to develop acute and chronic impairment
over one’s lifetime.[7] The illness places a considerable strain on
families, friends, and work settings.
While progress has been made in understanding the psychosocial
and behavioral mechanisms responsible for the development and maintenance of the
illness, there is an urgent need to optimize treatment approaches to reduce chronicity
and improve outcomes.[7] This necessitates new and innovative
treatments that contribute to long-term symptom reduction and incorporate contemporary
neurobiological findings such as those covered in TBT-S.
Key Point |
TBT-S has focused on AN because of its high mortality rate and low treatment efficacy over time. |
TBT-S Description
Temperament Based Therapy with Support (TBT-S) is an emerging neurobiologically
informed treatment approach designed to augment existing treatments. This course
describes how and why TBT-S has been developed for adults with AN, while recognizing
that it has the capacity to be applied to other psychological disorders. TBT-S
fills the gap between research and clinical practice by acknowledging and
treating underlying brain-based factors. TBT-S recognizes that there is a
biological basis to psychological illnesses that involves temperament and
altered brain function. This affects the regulation of eating and emotion for those
with AN. TBT-S applies neurobiological research findings to inform treatment
targets.
TBT-S combines psychoeducation and experiential activities that emphasize
the key role of neurobiological factors in the development and maintenance of AN
to increase insight and recognize temperament patterns. Skills-based training
is used to teach clients and Supports age-appropriate strategies to manage
these neurobiological factors so as to reduce problem thoughts and behaviors. TBT-S
treatment targets include common AN temperament traits (e.g., anxiety,
cognitive inflexibility, harm avoidance) and related brain processes such as
altered reward-and-punishment sensitivity, interoception, inhibitory control, and
decision-making.
The focus of TBT-S is to work with clients who have AN and their Support persons to
acknowledge, understand, and utilize their own temperament as a primary source
for strength and change. Supports can include members of one’s family of origin
(such as parents, siblings, grandparents, adult children) and of one’s “family
of choice” (such as spouses, partners, friends, housemates, or colleagues). The
TBT-S approach was developed and refined over a 10-year period, integrating AN
research with ongoing client and Support feedback to assure the intervention
strategies accurately reflect client experiences and temperaments.[8, 9] TBT-S was originally developed and studied in an intensive 5-day, 40-hour
program with groups of clients and their Supports.[9]
Key Point |
Temperament Based Therapy with Support (TBT-S) is an emerging and novel neurobiologically based treatment that works with a client's temperament to motivate change and to manage and reduce symptoms. |
What Is Temperament, and Why Is It Important?
Temperament is the biological basis of our personality, influenced
by genetics and brain circuit development and function over one’s life span. Character
is the external shaping of one’s temperament. Temperament is to nature as character is to nurture (Figure 1).
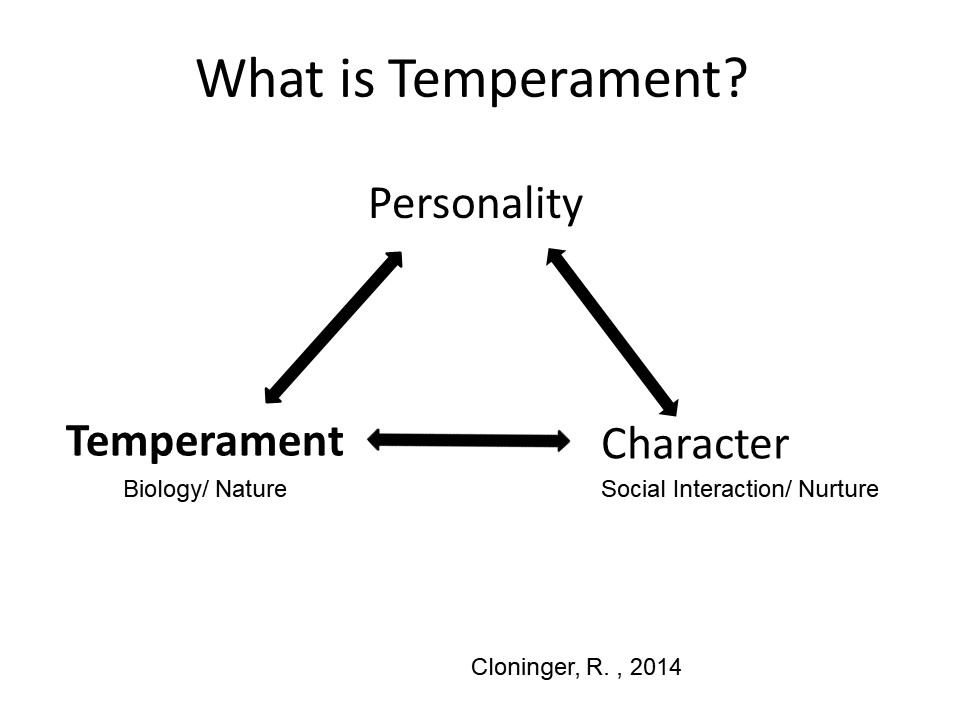
Figure 1. Temperament in relation to personality and character.
Temperament has been studied for more than 70 years with a
primary focus on children.[10] In the late 1980s Chess and Thomas led interventions for parents and educators to incorporate children’s “reactive
patterns” into classroom and parenting responses.[11] They countered the trend that children
were solely “products of the environment,” advocating that they bring their own
tendencies to the picture. Subsequently, temperament researchers began to acknowledge that traits can be disadvantageous in one situation and advantageous in others.[11] Educational and parental interventions encouraged a “goodness of fit” framework for children.[12] However, therapeutic interventions that focus on shaping adults’ “natural” thoughts, feelings, and behaviors have been
left off the therapeutic table in the area of eating disorders.[13, 14] Working with clients’ temperaments acknowledges who they are and what they bring of themselves to the therapeutic experience. (See Table 1.)
Table 1. What is Temperament? |
- The biological foundation to our personality
- Our innate (natural) features
- The genetic and neurobiological underpinnings that influence our thoughts, feelings, and behaviors over a lifetime.
Source: Cole (2020); Mitchell (2018)
|
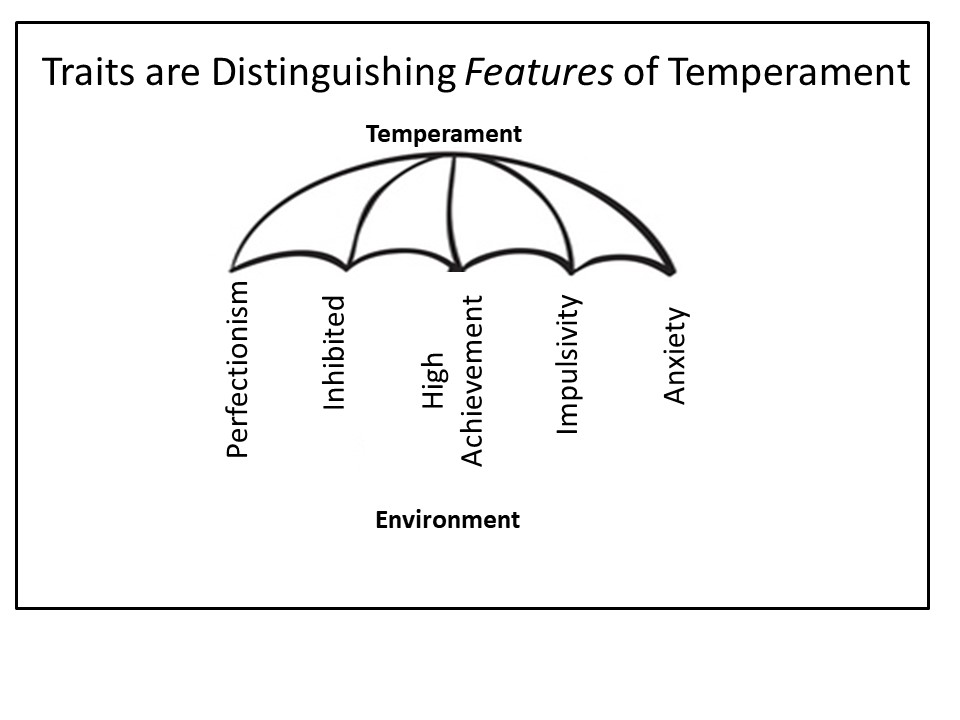
Figure 2. Traits are distinguishing features of temperament that interact with environment
Temperament is expressed through traits, as shown in Figure 2,
which affect our thoughts, feelings,
and behaviors. Temperament traits are observed in infancy and are relatively preserved across the lifespan, suggesting that personality is hardwired and consistent
throughout life. Importantly, temperament is strongly related to most
psychopathologies, especially those
involving anxiety and mood disturbance. People have varying levels of vulnerabilities
to develop a psychological disorder based on the traits they inherit. In fact, growing evidence indicates that temperament traits are uniquely associated with specific brain
systems linked to various psychopathologies, including those involved in Eating
Disorders (ED).[15–19] This suggests that temperament traits are genetic,
and brain-based, and have a powerful
influence on ED, and thus should be included in treatment approaches. (See Figure 3.)

Figure 3. Current ED therapies focus on personality and character
Key Point |
Temperament is the biological foundation of personality and consists of traits that are fundamental expressions of each person. |
Accumulating behavioral and neuroimaging evidence points to a
neurobiologically based AN
temperament that increases risk and contributes to the development and
maintenance of the disorder.[20–36] This AN temperament is characterized by anxiety, altered sensitivity to reward and
punishment, altered interoceptive awareness, difficulty with decision-making, and cognitive inflexibility
and rigidity.[30, 32, 37–42] Individuals with
AN also tend to be high-achieving,
perfectionistic, inhibited, and rule-abiding. These temperament and personality
traits are related to altered insula and fronto-striatal neural circuit function, highlighting their neurobiological basis.[43–47] In addition
to predating the disease, these traits often persist in a mild to modest degree after recovery, offering evidence they are biologically based traits and not behavioral symptom expressions.[30, 37–40, 48]
This AN temperament profile serves as a framework that
identifies the neurobiological constructs and traits targeted in TBT-S
and guides the interventions designed to address symptoms specific to AN.
TBT-S has been developed to fill a gap in ED treatment. It features
AN temperament, focusing on the traits that make a person vulnerable to AN, why
AN symptoms emerge and are maintained, and how to shift trait expressions or construct
environmental modifications to reduce symptoms and to impact positive change. (See
Figure 4.)

Figure 4. TBT-S augments other treatments by focusing on temperament
Key Point |
AN has common traits creating a temperament profile that guides TBT-S interventions to work with client traits as natural resources for lifelong changes. |
The theoretical model of TBT-S approaches the illness from the inside
out. It begins with genes. Environmental factors (such as life stresses, malnutrition,
and trauma) can modify gene expression and temperament via epigenetic processes
(e.g., gene x environment interactions), suggesting that although traits are
relatively stable, they can be shaped by experience and treatment.[49] Figure 5 shows the relationship between temperament and environmental influences
on symptoms. Genes, the center circle, code how the brain wires its circuits,
impacting thoughts, perceptions, feelings, and actions. Traits develop from
brain circuits structured by genes which are influenced by the environment.
Persons with AN have specific alterations in the wiring of these brain circuits
that contribute to destructive AN trait expressions.
Other circuits function normally, affording healthy and/or above-average
productive trait expressions. Altered trait expressions impact the type of
symptoms that develop. For example, elevated harm-avoidance is related to
dietary restriction and reduced social interactions. TBT-S focuses on
acknowledging and utilizing one’s trait expressions to modify, shape, and
promote recovery. For example, TBT-S prescribes structure and routine, in
alliance with a rule-bound trait, to reduce anxiety and intolerance of
uncertainty around meals. The inside-out approach of TBT-S complements ongoing therapies
that are grounded in environmental and behavioral models.

Figure 5. The relationship between traits and environmental influences on symptoms
Key Point |
The TBT-S theoretical model approaches treatment from the inside out, targeting traits and underlying biology that complement other treatment approaches which work from the outside in. |
Who Are the Intended Participants?
TBT-S was designed to be administered to adult clients and their
Supports. Thus, both clients and
Supports participate with the clinical team. Conducting TBT-S with clients and their Supports is a powerful and effective
way to ensure information is relayed, experienced, and processed similarly. We have focused our research and this course on adults with AN and their broad range of Supports in response to the higher
chronicity and mortality within this subpopulation. The TBT-S focus is on improving client-Support relationships and
communication to facilitate recovery. (See Table 2.)
Table 2. Temperament Based Therapy with Support (TBT-S) |
TBT-S is a treatment approach that:
- Works with clients’ nature, their temperament/traits.
- Explains the neurobiological underpinnings of client trait expressions.
- Draws on assistance from Supports for clients of all ages.
|
Key Point |
TBT-S endorses including Supports in the treatment of adults with anorexia nervosa to increase understanding of the illness and improve communication and continuity in care. |
Where Can TBT-S Be Applied?
TBT-S core principles and modules can be applied in (a)
one-on-one, (b) client with Support
person, and (c) client and/or Support group sessions either (d) virtually or
face-to-face, or (e) ranging from outpatient through day-hospital levels of
care. When TBT-S core principles are described in therapy sessions, clients
learn about the neurobiological underpinnings of their temperament expressions
and skills to help shape their traits. The therapeutic
change process is enhanced when additional components include virtual or face-to-face: (a) Support person(s), and
(b) the act of practicing the skills together. The learning and change process
can be further enhanced by providing TBT-S interventions in group settings through the power of client and Support interactions.[183]
TBT-S was originally developed in a 5-day group intensive format
to maximize efficacy, intensively build on skill development, minimize attrition, and
provide a practical and accessible approach for adult clients and Supports to work together in a discrete amount of time. Increased treatment frequency and
intensity are critical components
needed to elicit behavior change.[50, 51] Treatment
models for anxiety indicate that intense, repeated, and focused in vivo practice
is key to altering biologically driven avoidance behaviors by maximizing learning through massed practice and allowing close monitoring of compliance.[52–59]
Intensive treatment formats also show an increase in initial efficacy.[60, 61] This appears to be critical in treating AN, as evidence suggests that adolescents with AN who gain weight in the first four sessions of family-based treatment (FBT) have significantly better outcomes than
those who do not gain weight early in treatment.[62] An intensive
treatment format offers several
additional advantages, including reduced burden on the adult client and Support(s) of having to commit to
treatment over long periods of time, thus likely improving accessibility,
acceptability, and compliance. An initial intensive model may also be a cost-effective “jump-start” to shorten
residential or partial hospital treatments and augment outpatient ED treatments.
In the studied TBT-S 5-day model, multiple adult clients and
Supports are treated together in a group structure, commonly known as a multi-family group, in adolescent treatment.
Group settings enable and facilitate peer-to-peer consultation, a powerful method of learning that can improve outcomes. Having multiple adult clients and their Supports together can improve participants’ understanding of the illness by allowing them to learn from similar and diverse perspectives during group activities. Working with groups of clients and
Supports broadens viewpoints on effective ways to manage recovery and generates new ideas. The TBT-S focus is on
improving client-Support relationships and communication to facilitate recovery.
Key Point |
TBT-S was studied in a 5-day group format to intensify treatment intervention, unify clients and Supports, and increase accessibility to treatment. |
TBT-S Modular Structure
TBT-S is implemented as a modular treatment, meaning that it has
multiple, individual, complementary treatment interventions that have been
studied in different combinations as part of the 5-day TBT-S program. TBT-S
treatment modules were designed to target symptoms using a broad array of
intervention strategies (e.g., psychoeducation, experiential learning, skills training,
meal coaching and behavioral agreements) that include both the client and Supports.
Each TBT-S treatment module is described and includes a variety of
treatment activities. Clinicians can select activities from each module deemed
to be most relevant depending on the clinical presentations and developmental
stage of the clients and their Supports present in treatment.
Many clinicians may not have the infrastructure to deliver TBT-S
in its tested 5-day format. Individual treatment modules or activities can be
administered independently across multiple treatment settings, including
outpatient through partial hospitalization settings, and in multiple formats,
such as group, individual, or family therapy settings.
The TBT-S multi-day design has also been administered in shorter
intensive formats over two to four days in outpatient and higher level of care
settings in the United States, Canada, Norway, and Greece. Efforts to deliver
the multi-day TBT-S program in a
virtual format also appear promising. This course provides examples of how to structure and organize modules by treatment target or temperament trait in multiple treatment settings.
Key Point |
Clinicians can apply TBT-S flexibly, integrating its modular format with multiple treatment strategies to formulate unique stylized interventions. |
Two TBT-S Versions: Young Adult (YA) and Severe-and-Enduring Anorexia Nervosa (SE-AN)
Two versions of TBT-S have been developed and tested to date, YA
and SE-AN. Both versions uphold TBT-S
core principles as central themes and adhere to the same structure, format of treatment, and level of Support involvement. They differ in how adults are approached when in young adult stages of life development compared to adults who have Severe-and-Enduring forms of AN.
Young Adult TBT-S (YA TBT-S)
The Young Adult model of TBT-S (YA TBT-S) is designed for clients
with AN and other restrictive-type ED
between the ages of 17 and 27 and their parents, who are automatically nominated as primary Supports. This highly
focused version of TBT-S was designed to enhance treatment by integrating important developmental considerations since
many seeking treatment for AN often
fall within this age range. Naturally, young adults with AN are undergoing developmental changes and growth that are
central to this age and often have a
primary impact on treatment and recovery, both individually and within the context of their family system. YA TBT-S
is tailored to provide education on neurobiology, skills training, and a model
of family assistance that takes into account these important developmental considerations.
Emerging adulthood is a developmental window that has gained more
attention in recent years, in part because the incidence of mental illness is
highest in this developmental stage. Young adults do not squarely fit into either
adult or child/adolescent services because most in this age category are embarking
on the launch to independence (versus being fully independent) and, increasingly
so, continue to be embedded in their family system in important ways. Young adults
are adjusting to significant life transitions during this developmental stage, including
separation from family of origin, increasing autonomy and individual
responsibility, and more commonly in this modern era, interdependence within their
family of origin.
Developmentally, young adults are striving to individuate from
their family, learning to make their own decisions, and increasingly focusing on
carving their own path in life. This developmental backdrop is significant and imposing
in the life of a young adult and thus deserves consideration when working with clients
with AN in this age range. YA TBT-S brings these developmental dilemmas to the forefront
of treatment and addresses them within the context of recovery and treatment.
Themes touched on in treatment include: the capacity for change within
the context of the temperament framework due to neurodevelopment; how to assist
a YA in recovery from AN; how to make use of continued parental involvement to positively
impact recovery; how to strike a balance of autonomous and family-focused recovery;
and navigating an effective working relationship among YAs and their parents.
Severe-and-Enduring Anorexia Nervosa TBT-S (SE-AN TBT-S)
The SE-AN version of TBT-S is designed for all adults with AN across the life span who have chronic AN. It recognizes that
traditional adult therapy focuses on individuation. In contrast, TBT-S integrates interdependence within a
neurobiological framework. In this model, Supports may be anyone the client designates as a “support person.” The SE-AN version of TBT-S has been studied with clients of all ages, from newly graduated 18-year-old females and males to older clients in their 50s and 60s who have developed chronic AN tendencies. As SE-AN clients age, they tend to turn to a wider
diversity of Support persons, with
many of their primary family members having “burned out.”
Trait expressions continue
throughout one’s lifetime. When TBT-S is offered in a group format, the expertise
from older clients offers lived wisdom informing younger clients of symptoms
that can become ingrained over time,
while the younger clients resurrect hope and motivation in the older clients to reshape trait expressions. TBT-S presents neurobiological information that is congruent with AN temperament, increasing
awareness that there are tools that those with AN can utilize that align with their own temperament.
Clients tend to enter treatment assuming they have little within themselves that can be
a part of the solution. They report having tried many behavioral interventions, but some have failed over time. In a TBT-S
approach, the adult client educates, coaches, and clarifies with their Supports their own experiences of what it is like to have AN traits, how symptoms allow relief and lower anxiety, and what helps and does not help. Clients actively explore how to utilize the
same traits that have been expressed destructively in more productive ways.
The discovery that their authentic selves and their own
temperament have worth and are a means toward health and well-being motivates change and empowers their strengths. The more SE-AN adult clients align with the biological bases of their personality, the sooner they can
begin to identify how to use their own traits to impact change.
SE-AN adults have engrained, rule-bound rituals that have sustained their ED
symptoms over years. TBT-S utilizes its trait-based approach to empower the
rule-bound traits as solutions to step away from
destructive tendencies, using tools to shift the same traits toward productive expressions.
Key Point |
There are two versions of TBT-S. YA TBT-S is designed for ages 17–27 and integrates important developmental considerations into the TBT-S model. SE-AN TBT-S is designed for those aged 18–60 who have chronic AN symptoms (more than five years of illness). Both versions interrupt and shift AN symptoms by teaching clients to identify their own trait-based behavioral solutions. |
Summary Key Points |
- Temperament Based Therapy with Support (TBT-S) is an emerging neurobiologically informed treatment approach designed to augment existing treatments.
- TBT-S has been developed for adults with anorexia nervosa (AN), recognizing it has the capacity to be applied to other psychological disorders as well.
- TBT-S fills the gap between research and clinical practice by acknowledging and treating underlying brain-based factors.
- TBT-S recognizes that there is a biological basis to psychological illnesses that involves temperament and altered brain function.
|
TBT-S Core Principles
TBT-S has five core principles derived from neurobiological research:
- Eating disorders are brain and biologically based illnesses.
- Treat to the trait or the temperament underpinnings.
- Food is medicine.
- Supports are a necessary part of the treatment process.
- Action or movement is fundamental to change.
Eating Disorders Are Brain- and Biologically Based Disorders
TBT-S is grounded in the temperament based neurobiological
etiological model of anorexia nervosa (AN) initially developed by Kaye, et al.[35] and coined “When Good Traits Go Bad: Temperament and the Course of AN.” This model, as shown in Figure 6, recognizes AN as
a heritable illness with a strong genetic component.[6, 27, 28, 33, 63–66] Heritable risk is conferred through temperament traits that
increase susceptibility to developing AN and also serve to maintain the illness. This neurobiological model has been
updated to integrate findings from brain imaging studies showing altered function in brain systems regulating food intake in AN.
Key Point |
Key Point: Temperament traits and altered brain responses inform the treatment targets of TBT-S, which include altered anxiety, interoception, reward and punishment sensitivity, decision-making, and cognitive or inhibitory control. |
The updated neurobiological model shown in Figure 6 depicts
that good traits can go bad, and then
become good again. This is the TBT-S philosophy.
Approaching AN from a temperament based neurobiological perspective
provides a biological foundation and
conceptual framework from which to view symptoms and the underlying mechanisms that drive behavior. Temperament informs
targeted interventions directed at the cause of the behavior, rather than at the behavior itself. This is a paradigm shift for many. Treatment of AN has been thwarted by the lack of a mechanistic understanding of the disorder and recognition of the central role of temperament in its biological basis. This is similar to how
treatments of medical illnesses (like diabetes) were ineffective until the underlying mechanisms (insulin production) were discovered. Similarly, by adopting
a temperament based neurobiological and etiological model of AN, the treatment
emphasis shifts away from attempts to understand how behaviors developed and toward a focus on their functional impact to guidestrategies to redirect trait expressions to achieve a reduction
in eating disorder symptoms.

Figure 6. TBT-S neurobiological model of AN
Key Point |
TBT-S has emerged from a neurobiological model that identifies how “good” traits biologically shift to “bad” expressions and can become “good” again with trait-based intervention to promote recovery. |
Treat to the Trait: Targeting Temperament in Treatment
Individuals with AN often exhibit characteristic temperament traits. (See Table 3.) Some AN traits are productive and serve as strengths throughout
life. These traits can be utilized in the course of treatment to help clients manage
destructive traits. For example, many persons with AN are highly achievement-oriented,
which is needed to reduce ED symptoms and accomplish recovery. On the other
hand, some AN traits result from genetically induced, altered neural circuit
function that impacts the development and maintenance of the disorder.
As indicated in the TBT-S neurobiological model, ultimately, the
same traits that increase vulnerability to AN can be shifted from destructive expressions
that exacerbate ED symptoms to productive expressions that become strengths in overcoming
and maintaining a healthier and more successful lifestyle.
Table 3. Common Eating Disorder Traits |
- Obsessionality (symmetry, exactness)
- Sensitivity to criticism, punishment, mistakes
- Altered sensitivity to reward
- Anxiety, worry about what might happen (consequences), intolerance of uncertainty
- Harm avoidance, behaviorally inhibited
- Cognitive inflexibility, rule bound, difficulty with set shifting and decision-making
- Interoceptive awareness deficits
- Impulsive, emotionally reactive/dysregulated
|
It is important to note that not all people with AN will identify with all of the traits associated with
AN. Rather, these traits are like a menu, where most people with AN identify with at least a few, if not many or all, of these traits (see Table 3). Rather than trying to change traits that are hardwired in the brain (e.g., it would be difficult for an introvert to naturally become an extrovert), the goal of “treat to the trait” is to identify and experientially
explore how an individual’s traits could contribute to their strengths so as to
reduce their ED symptoms. TBT-S focuses on adjusting destructively expressed traits to expressions of strength by: (a) clients experientially identifying their own trait-based productive responses; (b) teaching skills to endorse client solutions; and (c) drawing upon Supports’ strategies to compensate for inherent difficulties.
The philosophy of TBT-S is to utilize “traits as strengths.”
Treatment modules and activities are
specifically designed to target one or more of the destructive trait
expressions and help clients realize how to shift them to strengths. This requires the clinician to adopt
what may be a different framework for conceptualizing these traits as strengths.
Table 4 provides an example of reconceptualizing traits as strengths and treatment
strategies that are used when treating to the trait.
Table 4: Reconceptualizing traits as strengths and strategies to treat to the trait |
| Trait |
Trait as strength
(productively expressed) |
TBT-S treatment strategy |
Uncertainty Intolerance |
Highly structured |
- Structure treatment
- Structure meal plan
- Identify explicit rules
|
| Altered sensitivity to reward/punishment |
Motivated by having options/ choices, planning, structure, and long-term goals |
- Offer multiple options instead of open-ended questions
- Structure plans
- Contingency management/nonnegotiables
|
| Obsessionality |
High error-detection
Attention to detail |
- Specific,
concrete rules
- Provide the details
|
| Anxiety |
- Thinks
about potential what-ifs
- thinks
through worst-case
- scenarios,
ability to plan and prepare
|
- Redirect, re-attend
- Stop, reboot, reroute
|
| Inhibition |
Ability to delay gratification, cautious, and unlikely to impulsively enter into harmful situation |
- Use long-term rewards and consequences via contingency management
|
Key Point |
Traits can be expressed destructively or productively, and clients can be taught to utilize their own traits as strengths throughout life. |
In discussing temperament, it is important to clarify differences
between traits and symptoms, highlighted in Table 5 and Figure 7. Symptoms are thoughts, feelings, and behaviors that have become problematic, dysfunctional, or harmful for persons and/or those around them. They are often
influenced by traits. For example, a person with a strong impulsive trait is more likely to develop a substance use disorder or engage in binge eating
than a person with an inhibited trait, who is more likely to avoid eating. ED symptoms, such as
food restriction, binge eating, purging, or excessive exercise, are behaviors
that can and should be eliminated. Temperament and traits, however, cannot be eliminated.
Table 5. How traits relate to symptoms |
Symptoms
- Are outward behavioral expressions
- Are indicators or reactions to illnesses
- Have the potential to be reduced and eliminated
Traits
- Are genetically programmed innate features
- Can be altered via intentionally shifting expressions
|

Figure 7. Example of trait impact on symptoms
Key Point |
Symptoms can be reduced or eliminated; traits are with us throughout life and vary in intensity. |
Food Is Medicine
Drawing from a biological perspective, food is the natural and
fundamental substance that “medicates”
our bodies to be strong, healthy, and balanced. Food is energy. Like other ED treatments, TBT-S recognizes that appropriate nutrition and body composition stabilization are necessary and fundamental to recovery. To
facilitate this, TBT-S includes comprehensive dietetic recommendations and meal plans “prescribed” by an ED dietitian.
The dietetic philosophy in TBT-S is that dosing energy for adults with AN is similar to dosing medicine. Clients and Supports attend dietary sessions and groups where they are “prescribed” foods and learn a meal plan tailored to the clients’ needs alongside other basic dietary information. Biological tenets of TBT-S are woven into the dietary philosophy by prescribing a dietary approach that acknowledges core personality and temperament traits and the biologically based function of recommended foods. TBT-S emphasizes a highly structured meal
plan in an effort to prioritize nutritional and weight rehabilitation in a way that
honors the AN client’s unique temperamental tendency toward structure and certainty.
Meal plans are organized to prioritize predictability and consistency. This can
include adherence to highly scheduled meal and snack times and predictable (and,
importantly, calorically sufficient) meals and snacks, among other things. In this
way, the treatment prioritizes structure and certainty over flexibility and variety
to cater to the clients’ preferences for structure based on personality.
TBT-S continues to acknowledge the need for dietary expansion,
which may include incorporating additional foods or expanding food horizons in a
variety of different ways. However, even this therapeutic endeavor toward variety
is approached in a structured manner.
Alongside Supports and the dietary team, clients learn to plan out
challenge foods in a structured format and, importantly, are the key stakeholders
in deciding how and when, and even if, this therapeutic endeavor is undertaken.
As such, TBT-S is unwavering in the need for abstinence from restriction and
ensures that clients adopt and practice a meal plan that is calorically sufficient,
includes major macronutrient groups, and upholds a more flexible approach with
regard to variety. This allowance stems from acknowledging that the need for
sameness and routine-surroundings eating may be related to core personality
styles and may in fact promote a more sustainable recovery practice in the long
term. This structure and routine around meals compensates for altered
interoception (e.g., altered hunger and/or satiety signaling that promotes food
restriction or overeating, altered trust in body-related signals),
decision-making (e.g., difficulty deciding what foods to eat), and reward sensitivity
(e.g., reduced brain response for pleasure to motivate eating and affirm how much
energy the body needs).
Key Point |
Food is framed as medicine for those with AN to integrate its biological purpose and “side effects,” and is “prescribed” in a structured format that schedules food variety based on client traits. |
Supports Are a Necessary Part of Treatment
TBT-S advocates that it is necessary to include Supports (spouses, parents, children of adult clients, roommates,
partners, friends, colleagues, etc.) in the treatment process for adults of all ages. The term “Supports” was chosen
at the request of clients participating in an open trial of TBT-S at The Center for Balanced Living, in Ohio, to reflect
their preference for support rather than being cared for, which they believed
the more common term “carer” connotes. TBT-S requires that a minimum of one Support person participate in
treatment with each client in designated sessions. Family-based treatment (FBT)
is the first-line treatment for adolescents with AN. It is effective
because it teaches families strategies to understand, interact, and manage AN.[67–69] Similarly, TBT-S focuses on providing psychoeducation and skills training so
that Supports learn about the causes of AN and effective ways to interact and
manage symptoms.
Supports are appointed as part of the treatment team and are seen
as an important asset to aid with recovery. The education, training, and
practice that they receive in TBT-S sessions are intended to increase empathy
and understanding by providing a biological understanding of AN and improving
their ability to provide effective assistance. Supports in TBT-S sessions
receive focused skills training on effective and age-appropriate assistance
strategies that are practiced throughout the clients’ treatment.
TBT-S takes the perspective that Supports play a critical role in recovery by
providing accountability, assistance, leverage, and the potential to compensate
for traits that clients do not have. Supports learn tools that the client
chooses as helpful to assist in the process of reducing ED symptoms. In addition to formal skills training, when TBT-S
is offered in group settings,
Supports also learn new skills by receiving feedback and consultation from both their loved one and other Supports,
as part of the TBT-S group milieu. If TBT-S is offered in a 5-day program, upon completion Supports are armed with what
the adult clients deem to be the best
practices for providing assistance, in the context of a biological and temperament perspective of the
illness. TBT-S views clients as the experts. Experts, however, do not work and function alone.
Key Point |
A Support is any person who offers support/assistance in a client’s life. Supports need the same information and tools as clients to offer consistency in reshaping altered trait expressions to promote recovery. |
Movement and/or Actions Are Fundamental to Change
TBT-S is a treatment of “doing.” The tendency to be physically active is one of the first traits to be identified historically and is considered the most essential trait of one’s temperament.[70] Behavioral change requires behavioral action. Learning occurs when “neurons
that fire together , wire together.”[50] Thus, our brains are fluidly flexible to change throughout life. The brain rewires through extensive practice of new ways of expression and behaviors, and
TBT-S capitalizes on this through guiding in vivo practice of new skills
during treatment. Clients and their Supports identify and practice the same
phrases and actions that they have identified as helpful toward achieving a healthier lifestyle.
Many of the TBT-S
treatment interventions are movement-driven; clients “try them on” to explore
new behaviors that bring them closer to their goals. Active interventions are helpful because the brain
learns through actions. Individuals are more likely to repeat what they have practiced. In vivo activities allow clients to refine their verbal and
behavioral responses through corrective feedback via their own experience or from that of others. This iterative method of corrective feedback serves to enhance building new skills.
Movement is also needed to shift cognitive sets. Many ED behaviors represent rituals that have become automatic. Many individuals with AN have a trait-based
tendency that causes their thoughts to become stuck on one topic. Movement can
be used to interrupt destructive thoughts and behaviors so as to shift and move
on to more productive thoughts and behaviors. TBT-S utilizes movement as a core part of the change process.
Key Point |
TBT-S is an active intervention approach. |
Summary Key Point |
TBT-S has five core principles that draw from neurobiological research to inform and direct treatment. |
Overview of Selected Intervention Strategies
TBT-S utilizes multiple intervention strategies to apply TBT-S
principles. These strategies have been developed and adapted over a 10-year period through iteratively integrating client and Support feedback in the treatment
development process to increase accuracy and acceptability. Five strategies are described in this section. It can be helpful to provide visual aids, including some of the figures in this course (detailed handouts are also available in the Appendices of the book).
Neurobiological Psychoeducation
The primary goals of neurobiological psychoeducation are to
educate clients and their Supports on
relevant neurobiological constructs, temperament traits, and associated symptom
expression and to provide a framework and rationale for TBT-S intervention
strategies. In doing so, neurobiological psychoeducation serves as an intentional strategy to increase motivation for recovery and
engagement in treatment, validate and reduce blame, and improve insight and awareness to inform skill-use and drive behavior change.
Psychoeducation materials include current genetic,
neurobiological, and biological research findings that address causes of Anorexia
Nervosa (AN) and introduce the neurobiologically based targets of treatment. These include the following
temperament traits: anxiety, altered interoception, sensitivity to reward and punishment, inhibitory control, cognitive flexibility, and decision-making.
This course provides scripts to help clinicians communicate neurobiological research in a standardized manner without requiring that they independently become neuropsychologists. We
describe relevant neurobiological information and key points for clinicians to
share with clients and their Supports.
Key Point |
Interactive psychoeducation identifies AN neurobiological underliers and offers a rationale for targeted interventions in a format all clinicians can utilize. |
Experiential Learning
TBT-S is a treatment of doing. This is accomplished through
carefully constructed experiential activities and in vivo practice,
conducted with clients and Supports in various treatment formats. Learning by doing heightens retention of information and facilitates skill-building. Practicing new skills and
behaviors during treatment, and developing solutions to problems rather than
just talking about them, increases the likelihood that clients and their Supports will continue to utilize the new skills and solutions in their daily lives.
Experiential Activities
TBT-S includes a series of experiential activities that are
designed to actively apply neurobiological information and elicit problem-solving strategies. They are intended to increase knowledge and empathy of Eating
Disorder (ED) behaviors and motivate change. These clinician-led experiential
TBT-S activities simulate AN experiences and temperament expressions through active metaphors to promote a better understanding of what it is like to live the illness, to experience and identify one’s own traits, and to help clients and Supports
identify and use methods congruent to their temperaments to solve problems.
Using game-like approximations of their AN experiences is a less threatening and acceptable approach to help clients work through solutions and compensatory strategies that
can be used to overcome and manage symptoms. Supports are included in the experiential activities sessions to learn about underlying causes and contributing factors of the illness at the same time as the clients. In addition, Supports are taught tools to develop skills that help their loved ones realize their potential outside of treatment and achieve success in symptom reduction.
Key Point |
Experiential treatment interventions provide frameworks for clients and their Supports to acknowledge and understand problems and explore solutions. |
Multi-Family Therapy (for Young Adult Version)
The Young Adult version of TBT-S includes approaches based on
multi-family therapy (MFT), where multiple clients and their families are
treated simultaneously in a group format. MFT has been shown to improve outcomes over single-family therapy.[71] In adult
AN, family therapy shows promise.[71] Additionally, considerable
evidence suggests that family interventions in adult mental health can be
enhanced by using a multi-family treatment format[73–75] and is feasible in adult AN.[76, 77] MFT is a powerful approach because it can enhance learning and change among clients and
their attending Supports and because attendees have the benefit of
learning from one another via sharing, feedback, modeling, and observation and comradery/group affiliation.
The Young Adult version of TBT-S considers the multi-family
milieu as a powerful opportunity to enhance change and recovery. Multi-family activities are used to facilitate
group cross-talk and sharing so that members have the opportunity to create a live assistance network consisting of others
with lived experience. Exercises emphasize creating affiliation and relationships and, later, interfamily feedback and peer-to-peer consultation so
that MFT group members have the opportunity to learn from one another.
Key Point |
Multi-family therapy is a powerful treatment format that can enhance outcomes. TBT-S has been applied and tested in a multi-family format. The Young Adult version of TBT-S includes a variety of multi-family therapy activities. |
Client and Support Skills Training
Clients and Supports receive skills training to develop tools
that can be used to reduce and manage symptoms and destructive or unhealthy trait expressions such as obsessive preoccupation with calories or food avoidance.
Client coping skills focus on constructive, temperament-congruent strategies targeting
symptom reduction. These include a variety of skills borrowed from other
treatment modalities such as dialectical behavior therapy (DBT), as well as skills developed to
target primary neurobiological targets such as anxiety and altered reward sensitivity.
Supports receive training on effective tools to assist their loved one. These tools address a variety
of factors that are common among Supports of individuals with AN, including tools that achieve a balance between providing emotional assistance and encouraging accountability. Support person skills also include a focus on developing
effective communication, demonstrating client-identified effective
responses to symptoms, reducing
blame, increasing empathy, and managing Support burnout.
In the 5-day program,
clients and Supports are separated for skills-training groups and receive training for effective management of ED symptoms in client-only or Support-only groups.
Key Point |
Clients and Supports receive focused skills training that integrate their own traits into skills development to manage and reduce client eating disorder symptoms. |
Meal Coaching and Dietary Activities
As noted in the core principles
section, TBT-S emphasizes action as a central treatment component. Treatment encourages in vivo practice, including therapeutic meals in various treatment settings. Clients and Supports and/or TBT-S clinicians attend the meals throughout treatment. The dietitian provides feedback and coaching as
necessary to navigate barriers to dietary success. The therapeutic meals may include the presence of ED behaviors such as restriction,
skills deficits to manage anxiety and other challenging experiences, and/or client/Support conflict or ineffectiveness.
In vivo meal practice and observation are necessary and active treatment components. Clinicians and dietitians remain present to make an assessment of interventions and skills
needed to increase success, and to observe client/Support patterns and any
emerging problematic behaviors. The
treatment team encourages clients and Supports to apply TBT-S skills learned during mealtimes, and intervenes as necessary to ensure that clients
and Supports alike are being skillful.
Dietitians are also present to ensure that clients are practicing the prescribed meal plan.
Clients are asked to make their meals and snacks, and dietitians “check off” on each meal and snack during treatment
to ensure that they are adequate and to provide feedback as necessary. Supports observe clients receiving feedback from dietitians. Additionally, they
practice providing learned TBT-S assistance strategies as necessary during designated meals and snack sessions.
Key Point |
Eating within structures with active coaching allows adult clients and Supports to practice taking their “medicines” in “doses” and combinations to meet individual needs. |
Framework for Action via the Behavioral Agreement
During TBT-S, clients and their Supports develop a written
Behavioral Agreement (BA) that establishes a mutually agreed -upon framework for necessary action that the client has identified so as to achieve recovery. The Behavioral Agreement is a written document – a treatment plan – that
includes daily commitments surrounding primary domains of recovery (such as eating or physical
activity) and a detailed plan for Support involvement.
There are two versions of the BA, the Severe-and-Enduring Anorexia
Nervosa (SE-AN) and Young Adult (YA) versions. They take slightly different approaches addressing differing developmental
stages and levels of Support involvement. The BAs are fundamental, structured
TBT-S clinician and client and Support tools to hold those with AN accountable and to develop and practice new client and Support skills. The BAs incorporate client temperaments to endorse congruence in client actions and client traits
Key Point |
Behavioral Agreements are structured frameworks for treatment plans developed to align with AN temperaments. |
Summary Key Point |
TBT-S structures its interventions around Behavioral Agreements for Young Adults (YA BA) and those with Severe-and-Enduring Anorexia Nervosa (SE-AN BA) that integrate experiential learning, meal planning/coaching, and skills training for clients and Supports. |
We now introduce the reader to two of the neurobiologically
informed modules to “try on” what could be shared with clients when explaining anorexia
nervosa and other eating disorders.
We have found that TBT-S could replace motivational treatments.
Adult and adolescent clients have repeatedly reported to us that once they
learn more details about the brain bases of their illness, guilt and oppressive
self-evaluations decrease, and knowledge about why they experience what they do
increases the desire to change. They report that they can picture what is
happening in their brain, why it is painful and hard to change, and yet report a
greater desire to change. TBT-S reflects and applies metaphoric parallels with Eating
Disorder brain responses to help clients use tools that compensate for what
they cannot do by themselves. This is not unlike wearing glasses. When retinal
neuropathways do not align correctly, many people need external glasses to
compensate for what cannot be seen clearly. TBT-S tools are clinical glasses to
compensate for what cannot be sensed internally or registered clearly in the
brain.
How to Deliver Neurobiology Psychoeducation as a Motivational
Strategy
Objective
The purpose of the Neurobiology Psychoeducation Modules are to
provide research evidence on anorexia nervosa (AN) as a neurobiological and
brain-based disorder. This evidence provides the neurobiological foundation, framework, and rationale for the neurobiologically based intervention strategies that have
evolved into a novel treatment approach called Temperament Based Therapy with Support (TBT-S).
Its specific goals follow:
- Introduce and provide educational information on relevant neurobiological constructs, temperament traits, and associated symptom expression.
- Offer a biologically based reason for hop eand increase motivation for recovery.
- Motivate engagement in treatment.
- Validate client/Support experience and reduce self/other blame.
- Improve client/Support insight and awareness of their own destructive/productive trait expression to inform skill use.
The Neurobiology Psychoeducation Modules are organized by
neurobiological and temperament
targets that are specifically addressed with temperament based
interventions. Clinicians can provide
these modules whenever deemed appropriate.
Who Is Involved
These psychoeducation modules are designed to be shared with
clients and/or their Supports in a
range of settings – including outpatient individual and group settings through higher levels of care – to educate clients
and/or their Supports on the neurobiological underpinnings of AN. Delivering psychoeducation in group settings offers the advantage of fostering discussion and sharing of experiences and knowledge among group members to facilitate communication and shared understanding.

Content
Content for each module on specific neurobiological
constructs and traits is provided in the following sections.
What Does the Research Say?
Several studies show benefits of providing psychoeducation to clients, their family members, and the community.[80–82] Importantly, this research suggests
that psychoeducational messages
emphasizing “malleable biology” and “cognitive-behavioral factors” tend to
produce more optimism and self-efficacy in recovery, as well as perceived
credibility of therapy compared with “biologically reductionist” messages that communicate that one’s psychological and emotional experience is
nothing more than the result of brain or biological functions.[81–85] In anxious individuals, biologically based psychoeducation has also been shown to reduce self-blame.[86]
However, clinicians should also be aware that studies have
identified factors associated with
poor outcomes following psychoeducation. These include psychoeducation that
takes an overly narrow and
reductionist biological etiological stance, and psychoeducation that is delivered solely via written text or
recorded videos, or involves assigning educational materials individually or online.[87, 88]
To maximize benefits, TBT-S psychoeducation is designed to be conducted by a clinician during a therapeutic session
with clients and/or Supports, encouraging questions and discussion, generating real-life examples, and providing validation of the clients’ experiences. TBT-S emphasizes neurobiological malleability and neuroplasticity. The brain can be
re-wired through behavioral practice and skill-use to manage AN traits and move toward recovery. As such, TBT-S
psychoeducation modules are used to increase understanding and motivation for
recovery, validate client experience when clinicians encourage clients to compare
their own experiences with research evidence, reduce Support blame and criticism,
and gain trust of and commitment to the TBT-S therapeutic interventions. Clients
report this increases their motivation to change their eating disorder (ED) symptoms.
Psychoeducation Module Instructions
Neurobiological psychoeducation in TBT-S is designed to be
delivered in an informal interactive lecture-style format. The content is
included in the following sections. The clinician role is to engage discussions
about individual experiences and knowledge in relation to the research findings.
This provides an opportunity for the clinician to correct misunderstandings
about ED such as inaccurate beliefs about the causes of AN (e.g., AN is a choice,
or the parents’ fault) and misattributions of the function of ED behaviors (e.g.,
food refusal is willful). This is best done by the clinician sharing the research
findings objectively and validating client/Support experiences. The
clinician can highlight the damage that misinformation causes (e.g., blame,
stigma).
This also serves to position the client as expert (consistent with
TBT-S philosophy) and facilitates open communication regarding knowledge
and beliefs about AN to align understanding and improve the client-Support relationship.
Clinician techniques and scripts (in italics) that can be used with all psychoeducation
modules follow:
1. Clinicians are encouraged to ask questions of the client and Support or group members to facilitate discussion and sharing of experiences.
- How do these findings compare with your own experience?
- Can you relate to these findings?
- How or what specifically resonates with your experience? What does not
resonate for you?
- Is there an example in your life that reflects these findings?
2. Clinicians solicit questions to tailor information to the specific needs and interests of the clients/Supports.
- How does this make sense, or not make sense to you?
- Do you have any questions about what has been covered today?
- What is your take-home message of this information in relation to your experience?
3. Clinicians acknowledge when they do not know an answer to a question.
- Full transparency is modeled by clinician authenticity and scientific
humility. This builds trust and fosters collaboration between clinicians and clients/Supports.
- Clinicians do not need to be experts in neurobiology to share neurobiological
research findings. Research is constantly growing.
- This course provides basic neurobiological information informing the
TBT-S approach. It is not exhaustive. If a clinician does not know an answer,
then the answer is, “I will look into that and find out.”
- The reference list at the end of the course may be helpful for clinicians
who would like to take a deeper dive into the scientific literature to share
with clients/ Supports.
4. Clinicians are encouraged to acknowledge limits to existing research and validate when the study findings do not match with an individual’s experience. If
the clinician is sharing research findings that they have read independently of the findings reported in this course, study limitations should be acknowledged. The findings described in this course take the limitations into account. Some common research limitations include the following:
- Results report averages across people in the study. It is expected that
individual client experiences may vary from the average findings reported.
- Many studies include a small number of clients in a homogenous group that
is not representative of the clients who are present for treatment. For
example, many studies are expected to not include clients who have comorbid diagnoses,
when in reality most clients have comorbid diagnoses such as depression, anxiety
disorders, trauma history, or substance abuse.
- Some studies do not differentiate between AN-restricting type and AN–binge/purge
type.
- Studies may address people at different states of illness (e.g., malnourished,
weight-restored but symptomatic, recovered), which can impact results.
5. Clinicians use neurobiological research as a foundation to engender hope that recovery is possible.
- Clinicians validate that treatment is difficult, and that clients may
feel counter to what they want to feel, due to their biological predisposition.
- You have to work harder than people who don’t have eating disorders to
eat in a healthier way. It is counter to the way you are hardwired. Your brain
signals are telling you not to eat, yet the best way to re-wire your brain is through
the practice of eating specified foods. You are swimming upstream, and you
are stronger by doing so.
Summary Key Points |
- Research indicates that providing biologically informed psychoeducation is beneficial to clients and their families.
- Psychoeducation that communicates that biology both contributes to AN and that biology can change to promote recovery is more effective than messages that only focus on the causative role of biology.
- TBT-S uses interactive psychoeducation as an interventional strategy to increase motivation for treatment and recovery, validate client/Support experience, reduce stigma and blame, and raise awareness of the role of temperament and neurobiology in maintaining eating disorder symptoms.
|
TBT-S Neurobiology Psychoeducation Module:
Anxiety and Interoception
Neurobiological and Trait Targets
- Anxiety
- Interoception
- Prediction Error (i.e., a mismatch between what is expected and what is experienced)
Objective
The purpose of the Anxiety and Interoception Psychoeducation
Module is to introduce clients and Supports to the scientific evidence
addressing the role of anxiety and altered interoception in disordered eating
behavior and other symptoms of AN. Interoception refers to disturbances in the experience of physical sensations inside one’s body. This module also provides the justification
and rationale for intervention strategies aimed at managing anxiety and
compensating for altered interoception by reducing reliance on internal (interoceptive)
signaling to promote healthy eating behavior.
When Is This Module Provided?
This module is provided early in treatment to set the stage for a
trait-based approach. However, it can be provided whenever the clinician wishes to introduce this topic. In the
studied 5-day TBT-S Programs, it was offered on the second day.
Who Is Involved
This module can be offered to clients only and/or Supports
only, individually or in a group. It was tested in a 5-day, 40-hour format with
a group of clients and their Supports to foster discussion and sharing of experiences among the group.
Content
The following six talking points and additional evidence are offered
for clinicians to share with clients
and Supports. Clinician scripts (which can be said verbatim) and notes
are provided to help guide discussion.
Point 1:
Individuals with AN Often Have High Anxiety[37, 104]
- Anxiety can be
cognitive (e.g., anxious thoughts, worry), physiological (e.g., stomach ache, nausea, difficulty breathing, racing heart), and/or anticipatory (fear of
upcoming event).
- Anxiety can be a state or a trait. If anxiety occurs rarely and only in a specific situation, it tends to be state anxiety. If the person experiences anxiety over various stages of life and has a tendency to feel overwhelmed and anxious over things, anxiety tends to be a trait.
- Forty percent of adults with AN had childhood anxiety disorders.
- In AN, eating is
associated with anxiety; food restriction or avoiding meals often serves to reduce anxiety.
- Anxiety in AN is associated
with:
- Lower BMI and greater caloric restriction
- More intense symptoms
- Poor outcome
- “Anxiety” genes (i.e., genes linked to anxiety are also associated with AN)
- Anxiety management is necessary to reduce symptoms of AN; TBT-S teaches skills to
effectively manage state and trait anxiety.
Point 2:
Role of Interoception in AN
- Interoception includes internal physical body-state experiences, such as hunger and fullness, taste, pain, touch, heartbeat, breathing, and gastrointestinal (GI) sensations.
- Many symptoms of AN relate to altered interoceptive experience, such as increased GI discomfort/distress, a disconnect between hunger/satiety and eating
behavior, and excessive exercise without experiencing much pain.
- Some of the earliest clinical descriptions of patients with AN are by Hilde Bruch, who in 1962 acknowledged “a failure of recognizing bodily states” as an important characteristic of the disorder, with disturbed perception of bodily sensations and distrust or inability to accurately identify feelings and sensations.
- Recent research indicates individuals with AN have
reduced trust in their body signals, and this distrust is related to worse eating disorder symptoms.[117]
Clinician Scripts
- Can you sense if you are hungry?
- Can you sense when you are full most of the time?
- Do you have a high pain threshold? Or, does it take intense pain before you tend to feel discomfort?
Notes for the Clinician
It can be helpful to discuss what the patient quote communicates,
including difficulty making sense of internal signals. Poor interoception leads to a sense of blindness or absence of guiding information. This makes it difficult to know what to expect of one’s self, and what the client needs from others (aka, Supports).
- Clarifying what to do when interoception is faulty is necessary. Clients and Supports can collaboratively set expectations and serve as guides. (A TBT-S structure to do this is through the Behavioral Agreements.
Point 3: The Insula Is Responsible for Interoception
- The insula is the area inthe brain that receives and evaluates interoceptive signals from the body
(taste, hunger, fullness, pain, touch) and integrates these signals with motivational/emotional information to
indicate if a person should approach or avoid various situations at any given time.
- The insula also includes the “gustatory cortex” or the region of the brain involved in processing taste.
- Brain imaging studies show that the insula functions differently in individuals with AN, often with
reduced response to interoceptive stimuli like taste and stomach sensations.[35,
45–47, 107]
Notes for the Clinician
- It can be helpful to present Figure 8.
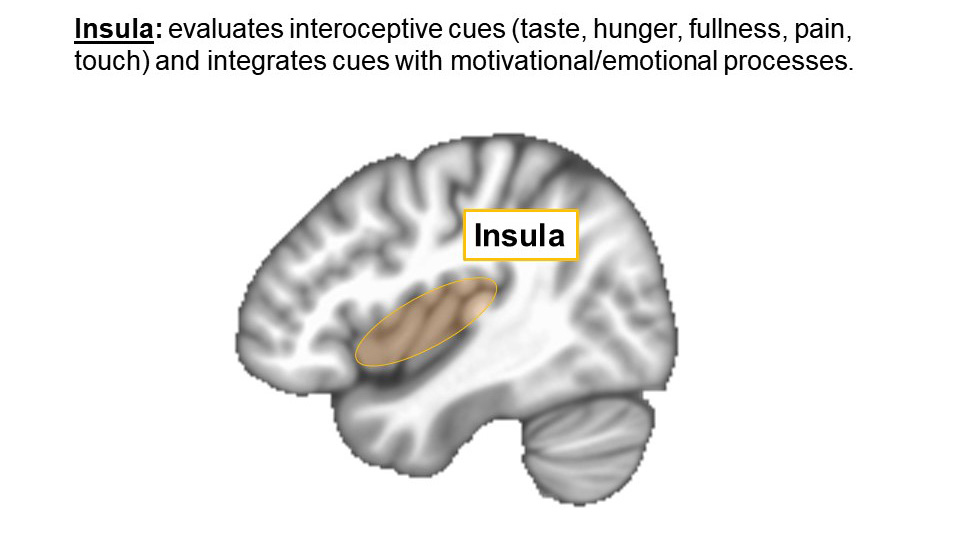
Figure 8. Insula
Point 4:
Individuals with AN Also Tend to Experience Interoceptive Prediction Errors
- A prediction error is the mismatch between what is expected and what is experienced.
- The ability to learn and adapt to one’s environment depends on the ability to accurately
predict outcomes using environmental cues.
- Learning occurs
through modifying expectations to meet experience (i.e., use feedback from the experience to modify the next
prediction and ultimately reduce the prediction error).
- An inability to make accurate predictions may impair learning from experience, explaining persistent engagement in maladaptive behavior.
- Several brain imaging studies show larger differences in the brain response during anticipation
versus receipt of an interoceptive experience (e.g., touch, restricted breathing, taste, pain). This suggests there is a brain basis for interoceptive prediction errors.[105, 106, 118–120]
An example of a neural interoceptive prediction error is shown in Figure 9.
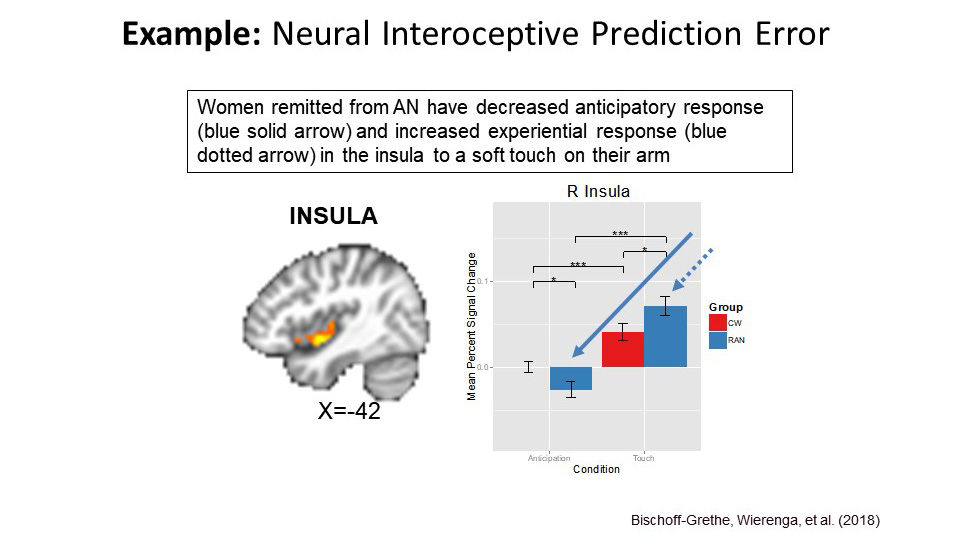
Figure 9. Example of a Neural Interoceptive Prediction Error
© The Author(s) 2018 Open Access. This article is licensed under a Creative Commons Atributin 4.0 International License, which permits use, sharing, adaptation, distribution, and reproduction in any medium or format, as long as you give appropriate credit t the original author(s) and the source, provide a link to the Creatie Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons license, unless indicted otherwise in a credit line to the material. If material is not included in the article's Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyight holder. To view a copy of this licens, visit http://creativecommons.org/licenses/by/4.0/.
Clinician Scripts
- Can you think of some real-world events in which what you expected did not match what you experienced? (Prediction Error).
- How did this impact your behavior? Did this trigger anxiety? Did it contribute to being
unsure of what to do?
- How has this caused you to modify your behavior?
Notes for the Clinician
- It can be helpful to provide examples of real-world prediction errors if the client or group has difficulty generating examples. Some examples follow:
- A person did not study for a test because they expected it to be easy and then
failed it.
- A person feels nervous about getting an injection only to experience it was not painful.
- A person worries about a meal, and it is not as bad as expected.
- It is also
helpful to discuss how this interoceptive mismatch or expectancy error informs future behavior. For example, does this cause someone to modify their behavior (i.e., learn from experience)? If so, why?
Point 5:
What Do Altered Interoception and Interoceptive Prediction Errors Feel Like to Someone with AN?
- Interoceptive prediction errors can make the world feel unpredictable. One client described her experience as follows: “I have no idea what to expect. I’m walking around blind. I look to others for guidance.”
- Altered interoception influences body distrust and/or body image disturbance.
- Altered interoception influences anticipatory anxiety and difficulty learning from experience.
- For example, one study showed that increased (altered) insula response
to touch anticipation was associated with greater harm avoidance and body dissatisfaction. This indicates that individuals with high harm-avoidance or body dissatisfaction have more acute altered anticipatory brain responses. This is shown in Figure 10.
- Altered interoception impacts avoidance behavior (e.g.,
avoidance of food or physical
changes), intolerance of uncertainty, and a need for structure.
- Deficits in internal brain signals necessitate reliance on external signals.
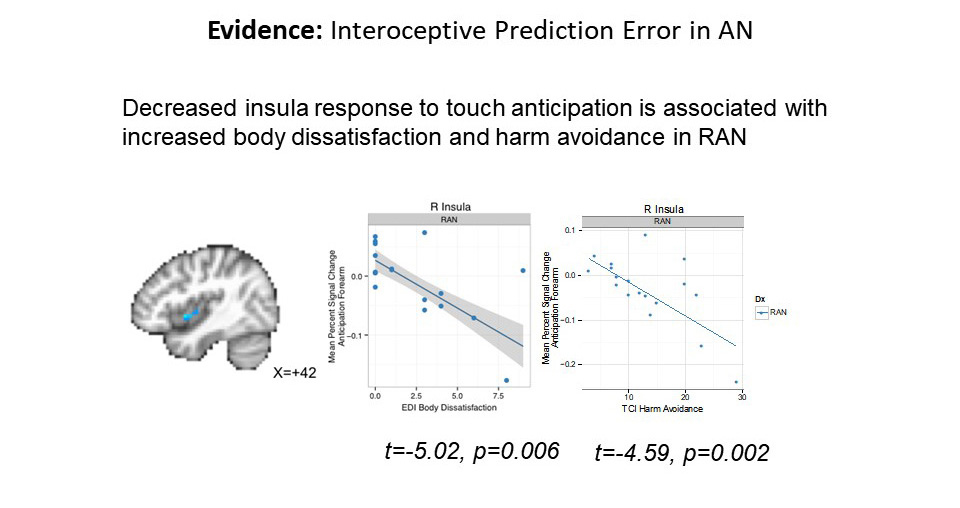
Figure 10. Decreased insula response to touch anticipation is associated with increased body dissatisfaction and harm avoidance in women remitted from anorexia nervosa
© The Author(s) 2018 Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution, and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
Notes for the Clinician
- It can be helpful to present Figure10.
Point 6:
How Does TBT-S Apply This Information to Treatment?
If one cannot rely on internal body-state signals, then it
is important for clinicians to use and encourage clients and Supports to:
- Rely on a predictable, external structure via meal plan
for food and creating specific plans for new events.
- Rely on advanced
planning of meals/snacks.
- Increase predictability
(reduce anxiety about uncertainty) through routine.
Key Point |
- Interoceptive prediction errors (mismatch between anticipation and experience of internal physical sensation) may relate to anticipatory anxiety, avoidant behavior, and difficulty learning from experience.
- Deficits in making sense of brain signals related to internal body experience suggest a reliance on external signals is needed as a means to achieve recovery.
|
TBT-S Neurobiology Psychoeducation Module:
Decision-Making and Inhibitory Control
Objective
The purpose of the Decision-Making and Inhibitory Control
Psychoeducation Module is to introduce clients and Supports to the scientific evidence demonstrating the role of altered
decision-making and inhibition in disordered eating behavior and other symptoms
of anorexia nervosa (AN). This module also provides the basis for strategies aimed at managing difficulties in decision-making and emphasizing that cognitive control can be redirected to promote healthy eating behavior.
When Is This Module Provided?
The module can be provided whenever the clinician wishes to introduce this topic. In the
studied 5-day format, it was provided on the third day in one program and on the second day in
another program.
Who Is Involved
This module can be offered to clients only and/or Supports only,
individually or in a group. It was tested in a 5-day, 40-hour format with a
group of clients and their Supports to foster discussion and sharing of experiences among the group.
Content
The following six talking points, as well as additional evidence,
are offered for clinicians to share with
clients and Supports. Clinician scripts (which can be said verbatim) and
notes are provided to help guide discussion.
Point 1:
Executive Functioning Is Often Altered in AN[110–113]
Performance on cognitive tasks suggests AN is characterized
by:
- Poor set shifting (e.g., stuck in set, perseveration, repetition of previous
behavior even if maladaptive)
- Difficulty task-switching (e.g., switching rules)
- Low central coherence (e.g., greater attention to detail, poor global
processing, losing the forest for the trees)
- Increased inhibitory control
- Altered decision-making (e.g., less risk-taking, less flexibility in adapting
to task demands)
Point 2:
The Cognitive Control Circuit Is Responsible for Executive Function
- The cognitive or inhibitory control circuit includes the
prefrontal cortex (PFC) and the dorsal (upper) part of the striatum, including the caudate nucleus. (See Figure 11.)
- It is involved in executive functioning, including
cognitive control, inhibition, planning and
decision-making (sometimes referred to as the CEO of the brain, since it
manages complex behavior).[101, 103]
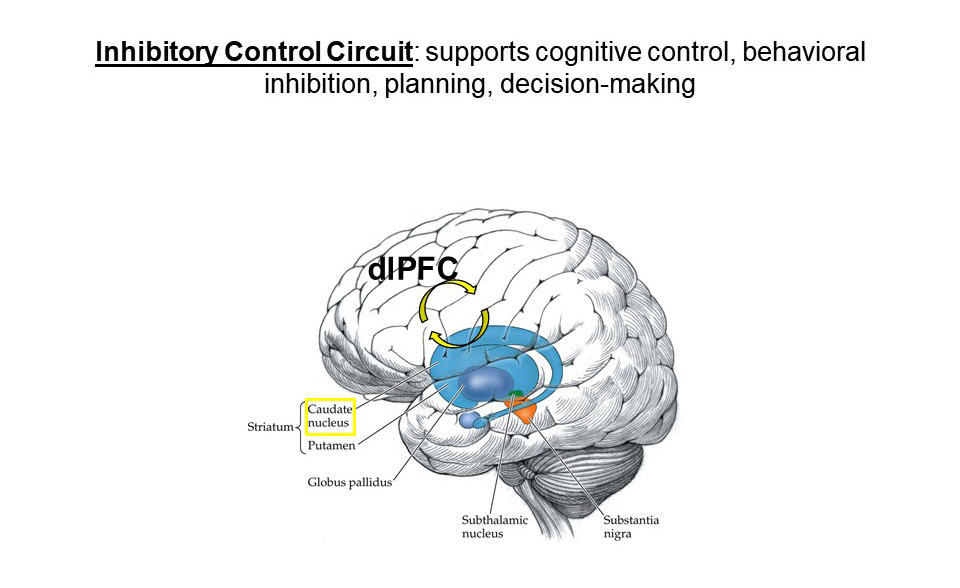
Figure 11. Inhibitory control circuit
Notes for the Clinician
- It can be helpful to present Figure 11.
Point 3:
Decision-Making Is Sometimes Altered in AN[47, 114, 115]
- Individuals with AN tend to be willing to wait longer for a bigger reward. For example, studies using
“delay discounting” decision-making tasks in the lab show that individuals with AN tend
to choose larger-later rewards
(like $20 in four weeks vs. $15
now) over smaller-sooner rewards (like $15 now vs. $20 in four weeks).
- In contrast, individuals with Bulimia Nervosa and impulse control disorders such as ADHD and substance-use disorders tend to prefer smaller-sooner rewards.
- This suggests individuals with AN are able to delay gratification and inhibit impulses/desires for immediate rewards in favor of perceived better long-term outcomes (this may help to explain the abilityto avoid immediately available food in favor of the long-term outcome of weight loss).
- Brain imaging studies show increased frontal brain response during
delay/discounting decision-making in individuals with a history of AN,
suggesting greater recruitment of cognitive control resources. In contrast,
individuals with AN show reduced brain reward response (in the ventral
striatum) to immediately available monetary reward, suggesting that AN may be
characterized by an imbalance between greater cognitive control/inhibition and
reduced reward sensitivity, which facilitates the ability to delay
gratification or avoid the temptation of something immediately rewarding,
such as food. (See Figure 12.)
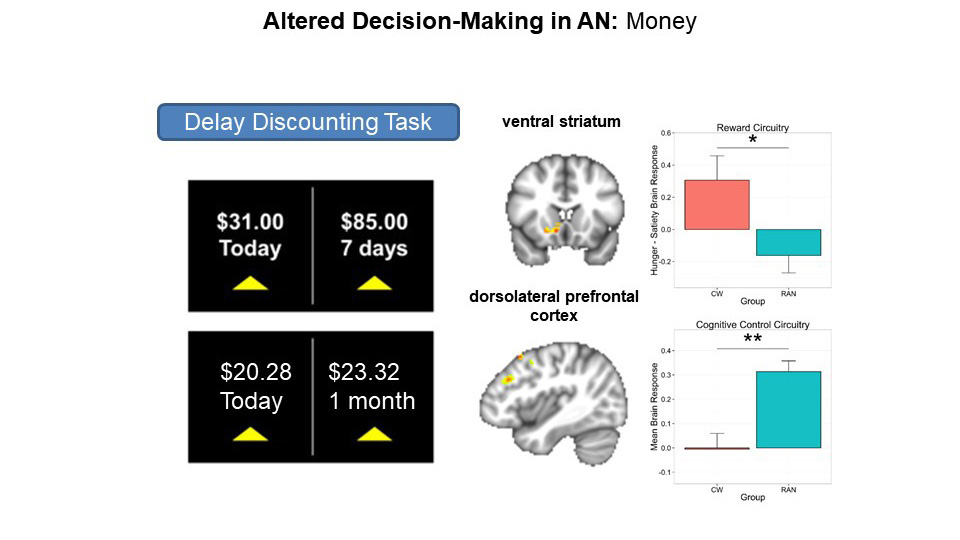
Figure 12. Altered brain response during decision-making in AN: Money
From Wierenga CE, Bischoff-Grethe A, Melrose AJ et al. Hunger does not motivate reward in women remitted from anorexia nervosa. Biol Psychiatr. 2015;77(7):642–52; and Ely A, Berner LA, Wierenga CE, et al. Neurobiology of Eating Disorders: Clinical implications. Psychiatr Times. 2016;33(4).
Notes for the Clinician
- It can be helpful to present Figure 12.
- “Delay discounting” is a neuroeconomics term that refers to the fact that humans tend to devalue money as time passes, so as the delay in receiving money increases, its value
is discounted. Delay discounting tasks are often used to assess impulsivity.
The preference of individuals with AN
who have restrictive traits to delay monetary rewards indicates that they do not discount its value as much after a
delay. In other words, they are not
impulsive; rather, they show great ability to inhibit immediate impulses.
- To engage clients and Supports, it can be fun to
demonstrate the task and have participants share their decision-making styles.
If clinicians opt to do this, it is recommended that this script be
provided prior to presenting the material in Point 3:
(Script) Delay-discounting tasks are commonly used to assess someone’s
decision-making style and whether they tend to be more impulsive or more
inhibited/restrained.
In this task, individuals must choose between two options of monetary reward: a
smaller-sooner reward or a larger-later reward. For instance, would you rather
receive $31 today or $85 dollars in four weeks? Raise your hand if you would
choose $31 today. Okay, now raise your hand if you would choose $85 in four
weeks. Those of you who chose $31, what motivated that decision? Those of you
who chose $85, what motivated that decision? What decision-making style do you
think individuals with AN, who are more restrictive, tend to use?
- To make these finding more relatable, the clinician
can ask the clients and Supports for real-life examples of this tendency to
delay gratification. Some examples may include rationing Halloween candy,
saving vacation days for a large trip in the future rather than using them on
more frequent (sooner) smaller trips, or saving up for a large purchase in the
future.
- Ask clients if they tend to inhibit an immediate impulse
and choose something that is considered of more value down the road, or vice
versa. This helps indicate whether their inhibition trait or impulsive trait is
stronger.
Point 4:
Individuals with AN Tend to Have Altered Decision-Making Regarding Food
- Not surprisingly, individuals with AN are more likely to choose low- versus high-calorie
food.[102]
- One study suggests that low-calorie food choices may be habit-driven. However, there is still debate in the field regarding the degree to which disordered eating behaviors are habit-based (automatic) or goal-directed (planned). This may depend on individual factors and length of illness (e.g., goal-directed behaviors can become habits over time). (See Figure 13.)
Notes for the Clinician
It can be helpful to present Figure 13.

Figure 13. Altered brain response during decision-making in AN: Food
From Foerde K, Steinglass JE, Shohamy D, et al. Neural mechanisms supporting maladaptive food choices in anorexia nervosa. Nat Neurosci. 2015;18(11):1571–3.
Point 5: What Do Altered Decision-Making and Greater Inhibition Feel Like to Someone with AN?
- One client described her experience as follows: “I get overwhelmed by the decision of what to eat. When there
are too many choices, I don’t know what is the right one, so I choose not to eat
because it’s easier than making the wrong
choice.”
- Increased cognitive control and behavioral inhibition may facilitate food avoidance and dietary restriction.
Notes for the Clinician
- It can be useful to recite the patient quote and ask the client or group what traits they recognize in the quote.
- The clinician can point out traits such as anxiety (“overwhelmed”), perfectionism (“the right one,” “easier than making the wrong choice”), interoceptive dysfunction (“I don’t know” suggests no physiological signaling of hunger or reward to
inform decision), inhibition (“choose not to eat”), and general difficulty in trusting a decision (“too many choices”).
Point 6:
How Does TBT-S Apply This Information to Treatment?
- Clinicians help clients and Supports set clear rules and
expectations for recovery-related behaviors (e.g., meal plan, types of movement
congruent with current body strength) to capitalize on the ability to follow rules (e.g., rule-bound behavior).
- Clinicians offer clients options to help them identify
motivating pro-recovery long-term rewards to take advantage of the ability to delay gratification.
- Clinicians and Supports offer multiple choices instead of open-ended questions to facilitate decision-making.
- Clinicians help clients and Supports plan ahead and avoid having to make new decisions on the spot.
- Clinicians use session time to practice new mealtime routines to re-wire destructive habit circuitry. Supports help clients practice these routines at home.
Summary Key Point |
- Eating disorders fundamentally involve disturbances in the experience of the physical sensations in one's body based on internal signals, referred to as interoception.
- Interoceptive prediction errors (mismatch between anticipation and experience of internal physical sensation) may relate to anticipatory anxiety, avoidant behavior, and difficulty learning from experience.
- Deficits in making sense of brain signals related to internal body experience suggest a reliance on external signals is needed as a means to achieve recovery.
|
Nondominant Hand:
TBT-S Neurobiological and Problem-Solving Experiential Activity
We strongly encourage the reader to “try on” the “Nondominant
Hand” activity while reading about it. The ‘doing’ of it brings a life to the
activity and allows enhanced comprehension for both the clinician and the
client.
Neurobiological and Trait Targets
These traits could work against the client in this situation:
- Altered interoception
- Altered reward sensitivity
- Anxiety
These traits could work for the client in this situation:
- Determination
- High achieving (or achievement oriented)
- Attentive/focused
- Persistence
Objectives
- Experience dominant destructive trait responses of ED thoughts and behaviors via a structured metaphorical activity.
- Experience how dominant destructive trait ED responses work against a person when overcoming ED symptoms.
- Identify what it takes to overcome dominant ED responses.
- Identify each client’s traits that helped them shift destructive ED traits to dominant
productive expressions.
Who Is Involved
- Clinician and ED client in one-on-one sessions virtually or face-to-face.
- Students in classroom.
- Clinician and ED clients and/or Supports in groups virtually or face-to-face.
Materials and Time Needed
- Paper and pencil/pen (not iPad or computer).
- 15 minutes.
The Nondominant Hand was first published in the Family Eating Disorder Manual, by Hill, L. et al., 2012, The Center for Balanced Living, Columbus, Ohio. A variation of it was also published in Brain-Based Approach to Eating Disorder Treatment, by Hill, L., The Center for Balanced Living, Columbus, Ohio. 2017.
What Does the Research Say?
- AN is associated with anxiety, decreased reward sensitivity, and altered interoception (i.e., experience of one’s internal physical sensations, such as
hunger) that serve to decrease motivation to eat.
- It is a “dominant” brain response to
enjoy food and eat with ease
for those who do not have eating disorders; it is
“nondominant” to experience pleasure, motivation, and hunger/fullness for those with ED.
- Altered brain circuits can be difficult to change, requiring that the brain
re-wires new circuits from repeated healthy actions to create new productive trait expressions.
Key Point |
Reducing ED symptoms is a nondominant brain response. |
Clinician Checklist
- Have the four steps of the activity memorized, do not read them. Conduct playfully.
- Draw upon client and/or Support answers; let them identify their own solutions.
- Memorize and
state the neurobiological and summary key points, looking at the clients directly
to enhance the points. Do not read them.
Experiential Activity Instructions
Rule
- The goal of this activity is to experience body responses,
thoughts, and feelings when an action is nondominant, by writing with the nondominant hand.
Steps and Scripts
1. Clinician shares (does not read) the following instructions:
- I would like you to try on
an experience that has you acting against your dominant responses that your
brain is wired to do.
- Please take out a piece of
paper and pencil/pen.
- There are four steps to this
activity.
2. Everything you write is
to be with your nondominant hand.
3. First, write down, with
your nondominant hand the following: “I am writing with my nondominant hand.”
- When completed: “Now show your writing
to the person next to you (or the clinician if one-on-one).”
- Allow a couple of minutes for each person to show what their writing looks like.
4. Now fill in the blank, your answer to this question, while writing with your nondominant hand: “I feel writing with my nondominant hand_________.”
- Wait while the client(s) and/or Supports write their “feeling words.
- No need to write the complete sentence.
5. Now turn to a person beside you as your partner (the partner would be the clinician in one-on-one settings). One person is to be the person who writes, the other person will be the “talker.”
When partners have identified their roles, present the following instructions:
- The person who is the talker is to speak to, interrupt, or disrupt in various ways the
person who is writing. Pressure the person to write faster and get done sooner.
- The person who is the writer is to write with their nondominant hand, the following statement, “I am still trying to write with my nondominant hand!”
- You have 30 seconds to write the above statement. Now begin.
When completed, instruct everyone to answer the last question using their nondominant hand.
- The last question, still using your nondominant hand, is: “If I were to tell you that you had to write with your nondominant hand for the rest of your life, what would you do?” (Note: not feel, or think, but do.)
- Wait
until everyone has completed their answers (about one minute).
How to Treat to These Traits
- Clinicians should use the client’s own solutions to respond to their ED symptoms.
- What was it like to show your “nondominant” writing to another person (NOT what did you feel)?
- This is similar to showing the results of your food logs to your clinician or dietitian.
- What did you “feel” when writing with your nondominant hand.
- Share responses.
- Empathically state out loud client and Support responses validating their voices; point out the feelings that are repeated, e.g., awkwardness.
- Ask clients if the feelings described are similar to what they feel when they try to eat their healthy meal plan.
- When interrupted by your partner, “what was it like to try to get the sentence
written in a short amount of time?”
- Empathically state out loud the clients’ and Supports’ responses, validating their voices.
- Ask clients if the responses are similar to what they experience when trying to eat their recommended meal when others are talking, interrupting, and pressuring them to hurry up.
- What did you write down that you would “DO” if told you had to use
your nondominant hand for the rest of your life?
- Empathically state out loud the clients’ and Supports’ responses, validating their voices.
- Use the clients’ and/or Supports’ own solutions. Some responses may include the following:
- “I wouldn’t write,
I’d find another way.” (This could be predictive of what the client is doing
with food intake.)
- “I’d practice” (the most frequent response). Practice is key.
- Clients want to eat and not feel upset, have fun and enjoy foods like others, exercise and not purge, but these are currently nondominant responses for them until they practice through or around them.
- Restricted
eating, or binge eating, or purging, or over-exercising are dominant, natural responses for those with ED.
- Every day requires ED clients to use nondominant actions to counter dominant brain responses. Not easy, not fun.
- Solutions are found in YOUR solutions that you gave, e.g., to repeatedly practice.
- The clients’ own traits can serve to shift dominant ED symptoms to healthy eating and exercise that can become more dominant over time with practice.
Key Point |
- Altered ED brain circuits contribute to the cause of dominant ED symptoms.
- For someone with AN, it is nondominant to eat the needed amount of food.
- It takes intense focus, practice, determination, and assistance to get through the distress of not doing the neurobiologically dominant ED actions.
|
Homework
Clients are to practice an action and their own productive traits
identified earlier for one week and report back.
Conclusion
This course introduces you to a new mental health treatment approach (TBT-S) that fills a significant gap by focusing on patients’ temperament traits, and research findings of underlying neurobiological irregularities that trigger symptoms. This approach holds the potential to be applied to other disorders that are trait based, such as anxiety or obsessive compulsive disorders. We have begun by focusing on eating disorders, specifically anorexia nervosa, due to the high rate of mortality and low rate of positive outcomes over time among adults.
TBT-S focuses on the root causes of an illness to augment ongoing therapies that concentrate primarily on symptoms. It treats from the inside out serving as the foundation for other treatments that treat from the outside in. Traits are central to who a person is and what their potentials are. TBT-S provides tools to help each client identify their own traits and how they are expressed on a continuum from productive to destructive. It provides tools to help clients use their productive traits to shift their destructively expressed traits to be the best of who they can be. It is critical for practitioners to know the difference between symptoms and traits since symptoms can be eliminated and traits are the means to manage and reduce symptoms throughout one’s life. TBT-S includes “Supports” in adult treatment integrating interdependence into treatment applications, ensuring that those who support the patient know the same information about the illness, have the same tools to use outside of treatment and learn when and how the client needs them for support.
TBT-S treats to the traits to manage symptoms with Supports for clients of all ages.
References
(Note: To return to the course after having clicked a footnote, click the Back button in your browser.)
1. Birmingham C, Su J, Hlynsky J, et al. The mortality rate from anorexia nervosa.
Int J Eat Disord. 2005;38:143–6.
2. Crow
S, Petersen C, Swanson S, et al. Increased mortality in bulimia nervosa and other eating disorders. Am
J Psychiatr. 2009;166:1342–6.
3. Foerde K, Steinglass J. Decreased feedback learning in anorexia nervosa persists after weight restoration. IntJEat Disord. 2017;50(4):415–23.
4. Udo T, Bitley S, Grilo C. Suicide attempts in US adults with lifetime DSM-5 eating disorders. BMC Med. 2019;17(1):120.
5. American Psychiatric
Association. DSM-5 Development. www.dsm5.org/Proposed Revision/Pages/proposedrevision.aspx? rid=26; 2012.
6. Bulik C, Blake L, Austin J. Genetics of eating disorders: What the clinician needs to
know. Psychiatr Clin North Am. 2019;42(1):59–73.
7. Zeeck A, Herpertz-Dahlmann B, Friederich H, et
al. Psychotherapeutic treatment for anorexia nervosa: A systematic review
and network meta-analysis. Front Psychiatr. 2018;9(158):1–14.
8. Hill L. Can Your Brain Cure Anorexia? A Brain-Based Approach to Eating Disorder Treatment Eating Disorders Catalogue. Carlsbad, CA: Gurze Books Publishing 2017.
9. Knatz Peck, S., Towne, T., Wierenga, C. E., Hill,
L., Eisler, I., Brown, T., Han, E., Miller, M., Perry, T., & Kaye, W. (2021). Temperament-based treatment for young adults with eating disorders: acceptability and initial efficacy of an intensive, multifamily, parent-involved treatment. Journal of eating disorders, 9(1), 110. https:// doi.org/10.1186/s40337-021-00465-x
10. Rothbart M. Advances in temperament, history, concepts and measures. In Zentner M, Shiner RL (Eds.), Handbook of Temperament (p. 3). New
York: Guilford Press; 2012.
11. Mervilde I, De Pauw
S. Models of child temperament. In
Zentner M, Shiner RL (Eds.), Handbook of Temperament (pp. 21–40). New York: Guilford Press; 2012.
12. Aron E. Temperament in psychotherapy: Reflections on clinical practice with the trait of sensitivity. In Zentner M, Shiner RL (Eds.), Handbook of Temperament (pp. 645–670). New York: Guilford Press; 2012.
13. Cole
C. Infant temperament predicts personality
more than 20 years later. Neuroscience News; 2020.
14. Mitchell K. Innate. Princeton, NJ: Princeton University Press;2018.
15. Whittle S, Allen N, Lubman D, et al. The neurobiological
basis of temperament: Towards a
better understanding of psychopathology. Neurosci Biobehav Rev. 2006;30(4):511–25.
16. Whittle
S, Yucel M, Fornito A, et al. Neuroanatomical correlates of temperament in early adolescents. J Am Acad Child Adolesc Psychiatr. 2008;47(6):682–93.
17. Yucel M, Harrison BJ, Wood S, et al. State, trait and biochemical influences on human anterior
cingulate function. Neuroimage. 2007;34(4):1766–73.
18. Hettema
J, Bourdon J, Sawyers C, et al. Genetic and environmental risk structure of internalizing psychopathology in youth. Depress Anxiety . 2020;37(6):540–8.
19. Tang A, Crawford H, Morales S, et al. Infant behavioral inhibition predicts personality and social outcomes three decades later. Proc
Natl Acad Sci USA. 2020;117(18):9800–7.
20. Kaye W, Bailer U. Understanding the neural circuitry of appetitive regulation in
eating disorders. Biol Psych. 2011;70(8):704–5.
21. Kaye
W, Wierenga C, Bailer U, et al. Nothing
tastes as good as skinny feels: The neurobiology
of anorexia nervosa. Trends Neurosci. 2013;36(2):110–20.
22. Kendler KS, MacLean C, Neale M, et al. The genetic epidemiology of bulimia nervosa. Am J Psychiatr. 1991;148 (12):1627–37.
23. Walters EE, Kendler KS. Anorexia nervosa and anorexic-like syndromes in a population-based female twin sample. Am J Psychiatr. 1995;152(1):64–71.
24. Lilenfeld L, Kaye W. Genetic studies of anorexia and bulimia
nervosa. In Hoek HW, Treasure JL, Katzman MA (Eds.), Neurobiology in the Treatment of Eating Disorders (pp. 169–194). Hoboken, NJ: John Wiley; 1998.
25. Strober M, Freeman
R, Lampert C, et al. Controlled family study of
anorexia nervosa and bulimia nervosa: Evidence of shared liability and transmission of partial syndromes. Am J Psychiatr.
2000;157 (3):393–401.
26. Treasure J, CampbellI. The casefor biology in the aetiology of anorexia nervosa. Psychol Med. 1994;24(1):3–8.
27. Berrettini W. Genetics of psychiatric disease. Annu Rev Med. 2000;51:465–79.
28. Bulik C, Sullivan PF, Tozzi F, et
al. Prevalence, heritability and prospective risk factors for anorexia nervosa. Arch Gen Psychiatr. 2006;63(3):305–12.
29. Steinglass JE, Walsh T. Psychopharmacology of anorexia nervosa, bulimia nervosa, and binge eating disorder. In Brewerton TD (Ed.), Clinical Handbook of Eating Disorders:
An Integrated Approach (pp. 489–508). New York: Marcel Dekker; 2004.
30. Anderluh MB, Tchanturia K, Rabe-Hesketh S,etal. Childhood obsessive-compulsive personality traits in adult women with eating disorders: Defining a broader eating disorder phenotype. Am
J Psychiatr. 2003;160(2):242–7.
31. Stice E. Risk and maintenance factors for eating pathology: A meta-analytic review. Pychopharmacol Bull. 2002;128:825–48.
32. Lilenfeld L, Wonderlich S, Riso LP, et al. Eating disorders and personality: Amethodological and empirical review. Clin Psychol Rev. 2006;26(3):299–320.
33. Bulik
C, Breen G. Solving the eating disorders
puzzle piece by piece. Biol Psychiatr. 2017;81(9):730–1.
34. Wadden T, Sternberg J, Letizia K, et al. Treatment of obesity by very low calorie diet, behavior therapy, and their combination: A five-year perspective. Int J Obes. 1989;30(Suppl 2):39–46.
35. Kaye W, Fudge J, Paulus M. New insights into symptoms and neurocircuit function of anorexia nervosa. Nat Rev Neurosci. 2009;10(8):573–84.
36. Kaye W, Wierenga C, Bailer U, et al. Does a shared neurobiology for foods and drugs of abuse contribute to extremes of food ingestion in anorexia and bulimia nervosa? Biol Psychiatr. 2013;73(9):836–42.
37. Kaye
W, Bulik C, Thornton L, et al. Comorbidity of anxiety disorders with anorexia and bulimia nervosa. Am J Psychiatr. 2004;161(12):2215–21.
38. Cassin
S, von Ranson K. Personality
and eating disorders: A decade in review. Clin Psycho Rev. 2005;25(7):895.
39. Wagner A, Barbarich N, Frank G, et al. Personality traits after recovery from eating disorders: Do subtypes differ? Int J Eat Disord. 2006;39(4):276–84.
40. Lilenfeld L. Personality and temperament. Curr Top Behav Neurosci. 2011;6:3.
41. Fassino
S, Piero A, Gramaglia C, et al. Clinical,
psychopathological and personality correlates of interoceptive awareness in anorexia nervosa, bulimia nervosa and obesity. Psychopathology. 2004;37(4):168–74.
42. Harrison A, O’Brien N, Lopez C, et al. Sensitivity to reward and punishment in eating disorders. Psy Res. 2010;177 (1–2):1–11.
43. BernerL, Crosby RD, Cao, L, et al. Temporal associations between affective instability and dysregulated eating behavior in bulimia nervosa. J Psychiatr Res. 2017;92:183–90.
44. DeGuzman
M, Shott M, Yang T, et al. Association of elevatedreward prediction error response with weight gain in adolescent anorexia nervosa. Am J Psychiatr . 2017;174(6):557–65.
45. Kerr K, Moseman S, Avery J, et al. Altered insula activity during visceral interoception in weight-restored patients with anorexia nervosa Neuropsychopharmacology. 2016;41 (2):521–8.
46. Oberndorfer T, Frank G, Fudge J, et al. Altered insula response to sweet taste processing after recovery from anorexia and bulimianervosa. Am J Psychiatr. 2013;214(2):132–41.
47. Wierenga C, Bischoff-Grethe A, Melrose A, et al. Hunger does not motivate reward in women remitted from anorexia nervosa. Biol Psychiatr. 2015;77(7):642–52.
48. Atiye M, Miettunen J, Raevuori-Helkamaa A. A meta-analysis of temperament in eating disorders. Eur Eat DisordRev. 2015;23(2):89–99.
49. Steiger H, Booij L. Eating disorders, heredity and environmental activation: Getting epigenetic concepts into practice. J Clin Med. 2020;9(5):E1332.
50. Hebb D. The Organization of Behavior. New York: McGraw-Hill; 1949.
51. Kolb B. Brain Plasticity and Recovery of Function in Adulthood. Mahwah, NJ: Lawrence Erlbaum Associates; 1995.
52. Abramowitz
J, Foa E, Franklin M. Exposure and ritual prevention for obsessive-compulsive disorder: Effects of intensive versus twice-weekly sessions. J Consult Clin Psychol. 2003;71(2):394–8.
53. Deacon
B, Abramowitz J. A pilot study of two-day cognitive-behavioral therapy for panic disorder. Behav Res Ther.2006;44 (6):807–17.
54. Gallo
K, Chan P, Buzzell B, et al. The impact of an eight-day intensive treatment for adolescent panic disorder and agoraphobia on comorbid diagnosis. Behav Ther. 2012;43:153–9.
55. Ollendick T, Ost L, Reyuterskiold L, et al. One-session treatment of specific phobias in youth: A randomized clinical trial in the United States and Sweden. J Consult Clin Psychol. 2009;77:504–16.
56. Santucci
L, Ehrenreich J, Trosper S, et al. Development and preliminary evaluation of a one-week summer treatment program for separation anxiety disorder. Cogn Behav Pract. 2009;16:317–31.
57. Schmidt
R, Bjork R. New conceptualizations of practice: Common principles in three paradigms suggest new concepts for training. Psychol Sci. 1992;3 (4):207–17.
58. Storch E, Geffken G, Merlo L,et al. Family-based cognitive-behavioral therapy for pediatric obsessive-compulsive disorder: Comparison of intensive and weekly approaches. J Am Acad Child Adolesc Psychiatr. 2007;26:469–78.
59. Whiteside S, Jacobsen A. Anun controlled examination of a 5-day intensive treatment for pediatric OCD. Behav
Ther. 2010;41:414–22.
60. Fernandez M, Storch E, Lewin A, et al. The principles of extinction and differential reinforcement of other behaviors in the intensive cognitive-behavioral treatment of primarily obsessional pediatric OCD. Clin Case Stud. 2006;12:511–21.
61. Storch E, Merlo L, Lehmkuhl L, et al. Cognitive-behavioral therapy for obsessive-compulsive disorder: A non-randomized comparison of intensive and weekly approaches. J Anxiety Disord. 2008;22(7):1146–58.
62. Doyle P, Le Grange D, Loeb K, et al. Early response to family-based treatment for adolescent anorexia nervosa. Int J Eat Disord. 2010;43(7):659–62.
63. Bulik C M, Devlin B, Bacanu S A, et al. Significant linkage on chromosome 10p in families with bulimia nervosa. Am J Hum Genet. 2003;72(1):200–7.
64. Bulik C M, Sullivan PF, Kendler KS. Heritability of binge-eating and broadly defined bulimia nervosa. Biol Psychiatr. 1998;44(12):1210–8.
65. Duncan L, Yilma Z, Gaspar H, et al. Significant
locus and metabolic genetic correlations revealed in
genome wide association study of anorexia nervosa. Am J Psychiatr. 2017;174(9):850–8.
66. Hinney
A, Kesselmeier M, Jall S, et al. Evidence for three
genetic loci involved in both anorexia nervosa risk and variation of body mass index. MolPsychiatr. 2017;22 (2):321–2.
67. Lock J, Le Grange D. Can family-based treatment of anorexia nervosa be manualized? J Psychother Pract Res. 2001;10(4):253–61.
68. Lock J, le Grange D. Family-based treatment of eating disorders. Int J Eat Disord. 2005;37(Suppl):S64–S7.
69. LoebK, LeGrange D. Family-based treatment for adolescent eating disorders: Current status, new applications and future directions. Int J Child Adolesc Health. 2009;2(2):243–54.
70. Strelau J, Zawadzki B. Activity as a temperament
trait. In Zentner M & Shiner RL
(Eds.), Handbook of Temperament (pp.
83–104). New York: Guilford Press; 2012.
71. Eisler I, Simic M, Hodsoll J, et al. A pragmatic randomised multi-centre trial of multifamily and single family therapy for adolescent anorexia nervosa. BMC Psychiatr. 2016;16(1):422.
72. Dare
C, Eisler I, Russell G, et al. Psychological therapies for adults with anorexia nervosa: Randomised controlled trial of out-patient treatments. BR J Psychiatr. 2001;178:216–21.
73. Lemmens
G, Eisler I, Buysse A, et al. The effects on mood of adjunctive single family and multi-family group therapy in the treatment
of hospitalised patients with major depression: An RCT and 15 months follow-up
study. Psychother Psychosom. 2009;78:98–105.
74. McFarlane W. Family interventions for schizophrenia and the psychoses: A review. Fam Process. 2016;55(3):460–82.
75. Miller I, Solomon CE, Keitner G. Does adjunctive family therapy enhance recovery from bipolar I mood episodes? J Affect Disord. 2004;82(3):431–6.
76. Dimitropoulos G, Farquhar J, Freeman V, et al. Pilot study comparing multi-family therapy to single family therapy for adults with anorexia nervosa in an intensive eating
disorder program. Eur Eat Disord Rev. 2015;23(4):294–303.
77. Tantillo M. A relational approach to eating disorders multifamily therapygroup: Moving from difference and disconnection to mutual connection. Families Syst Health. 2006;24(1):82–102.
78. Kaye W, Wierenga C, Knatz S, et al. Temperament-based treatment for anorexia nervosa. Eur EatDisordRev. 2015;23(1):12–18.
79. Hill L, Peck S, Wierenga C, et al. Applying neurobiology to the treatment of adults with anorexia nervosa. JEat Disord. 2016;4:31.
80. Crisafulli M, Von Holle A, Bulik C. Attitudes towards anorexia nervosa: The impact of framing on blame and stigma. Int J Eat Disord. 2008;41(4):333–9.
81. Wiesjahn M, Jung E, Kremser J, et al. The potential of continuum versus biogenetic beliefs in reducing stigmatization against persons with schizophrenia: An experimental study. JBehav TherExp Psychiatr. 2016;50:231–7.
82. Hod Y. Psychoducation des patients et de leurs proches dans les pisodes psychotiques [Psychoeducation of patients and their family members during episode psychosis]. Encephale. 2013;39(Suppl 2): S110–S4.
83. Farrell
N, Lee A, Deacon B. Biological or psychological? Effects of eating disorder psychoeducation on self-blame and recovery expectations among symptomatic individuals. Behav Res Ther. 2015;74:32–7.
84. Lebowitz
M, Ahn W. Emphasizing malleability in the biology
of depression: Durable effects on perceived agency and prognostic pessimism. Behav Res Ther. 2015;7:125–30.
85. Han D, Chen S.Reducing the stigma of depression through neurobiology-based psychoeducation: A randomized controlled trial. Psychiatr Clin Neurosci. 2014;68(9):666–73.
86. Lebowitz, M S, Pyun, J J., Ahn, W.K. Biological explanations of generalized anxiety disorder: effects on beliefs about prognosis and responsibility. Psychiatr Serv. 2014;65(4):498–503.
87. Lebowitz M, Ahn W, Nolen-Hoeksema S. Fixable or fate? Perceptions of the biology of depression. J Consult Clin Psychol. 2013;81(3):518–27.
88. Zimmermann
M, Papa A. Causal explanations of depression and treatment credibility in adults with untreated depression: Examining attribution theory. Psychol Psychother. 2020;93(3):537–54.
89. Lilenfeld LR, Kaye WH, Greeno CG, et al. A controlled family study of
anorexia nervosa and bulimia nervosa: Psychiatric disorders in first-degree relatives and effects of proband
comorbidity. Arch Gen Psychiatr. 1998;55(7):603–10.
90. Bulik C, Slof-Op’t Landt M, van Furth E, et al. The genetics of anorexia nervosa. Ann Rev Nutr. 2007;27:263–75.
91. Watson
H, Yilmaz Z, Thornton LH, et al. Genome-wide
association study identifies eight risk loci and implicates metabo-psychiatric
origins for anorexia nervosa. Nat Genet. 2019;51(8):1207–14.
92. Klump K, Strober M, Johnson C, et al. Personality
characteristics of women before and after recovery from an eating disorder. Psych Med. 2004;34(8):1407–18.
93. Jacobs M, Roesch S, Wonderlich S, et al. Anorexia nervosatrios: Behavioral profiles of individuals with anorexia nervosa and
their parents. Psychol Med. 2009;39(3):451–61.
94. Woodside DB, Bulik CM, Halmi KA, et al. Personality, perfectionism, and attitudes toward eating in parents of individuals with eating disorders. Int J Eat Disord. 2002;31(3):290–9.
95. Harrison A, Sullivan S, Tchanturia K, et al. Attentional bias, emotion recognition and emotion regulation in anorexia: State or trait? Biol Psych. 2010;68(8):755–61.
96. Klump K, Keel P, Racine S, et al.The interactive effects of estrogen and progesterone on changes in emotional eating across the menstrual cycle [Errata]. J Abnorm Psychol. 2013 Feb;122(1):137.
97. Klump
K, Fowler N, Mayhall L, et al. Estrogen moderates genetic influences on binge eating during puberty: Disruption of normative processes? J Abnorm Psychol. 2018;127(5):458–70.
98. Berthoud H, Lenard N, Shin A. Food reward, hyperphagia, and obesity. AM J Physiol Regul IntegrComp Physiol. 2011;300(6):R1266–R77.
99. Cowdrey
F, Park R, Harmer C, et al. Increased neural processing of rewarding and aversive food stimuli in recovered anorexia nervosa. Biol Psych.
2011;70 (8):736–43.
100. Frank G, Reynolds J, Shott M, et al. Anorexia
nervosa and obesity are associated with opposite brain reward response. Neuropsychopharmacology. 2012;37(9):2031–46.
101. Lock J, Garrett A, Beenhakker J, et al. Aberrant brain activation during a response inhibition task in adolescent eating disorder subtypes. Am J Psychiatr. 2011;168(1):55–64.
102. Foerde K, Steinglass J, Shohamy D, et al. Neural mechanisms supporting maladaptive food choices in anorexia nervosa. Nat Neurosci. 2015;18(11):1571–3.
103. Ehrlich S, Geisler D, Ritschel F, et al. Elevated cognitive control over reward processing in recovered female patients with anorexia nervosa. JPsychiatr Neurosci. 2015;40(5):307–15.
104. Dellava
J, Thornton L, Hamer RS, et al. Childhood anxiety associated with low BMI in women with anorexia nervosa. Behav Res Ther. 2010;48(1):60–7.
105. Bischoff-Grethe A, Wierenga C, Berner L, etal.Neural hypersensitivity to pleasant touch in women remitted from anorexia nervosa. Transl Psychiatr. 2018;8(1):161.
106. Holsen L, LawsonE, Blum K, et al.Food motivation circuitry hypoactivation related to hedonic and nonhedonic aspects of hunger and satiety in women with active anorexia nervosa and weight-restored women with anorexia nervosa. J Psychiatr Neurosci. 2012;37(5):322–32.
107. Kaye W, Wierenga C, Bischoff-Grethe A, et
al. Neural insensitivity to the effects of hunger in women remitted from anorexia nervosa. Am J Psychiatr. 2020;177 (7):601–10.
108. Bischoff-Grethe
A, McCurdy D, Grenesko-Stevens E, et
al. Altered brain response to reward and punishment in adolescents with anorexia nervosa. Psychiatr Res. 2013;214 (3):331–40.
109. Frank G, Collier S, Shott M, et al. Prediction error and somatosensory insula activation in women recovered from anorexia nervosa. J Psychiatr Neurosci. 2016;41(2):304–11.
110. Roberts
M, Tchanturia K, Stahl D, et al. A systematic review and meta-analysis of set-shifting ability in eating disorders. Psychol Med. 2007;37(8):1075–84.
111. Smith
K, Mason T, Johnson J, et al. A systematic review of reviews of neurocognitive functioning in eating disorders: The state-of-the-literature and future
directions. Int J Eat Disord. 2018;51 (8):798–821.
112. Wu M, Brockmeyer T, Hartmann M, et al. Set-shifting ability across the spectrum of eating disorders and in overweight and obesity: A systematic review and meta-analysis. Psychol Med. 2014;44 (16):3365–85.
113. Berner L, RomeroE, Reilly EE, et al. Task-switching inefficiencies in currently ill, but not remitted anorexia nervosa. Int J Eat Disord. 2019;52 (11):1316–21.
114. Decker J, Figner B, Steinglass J. On weight and waiting: Delay discounting in anorexia nervosa pretreatment and post-treatment. Biol Psychol. 2015;78 (9):606–14.
115. Steward
T, Mestre-Bach G, Vintro-Alcaraz C, et al. Delay discounting of reward and impulsivity in eating disorders: From anorexia nervosa to binge eating disorder. Eur Eat Disord Rev. 2017;25(6):601–6.
116. Wierenga
C, Ely A, Bischoff-Grethe A, et al. Are extremes of consumption in eating disorders related to an altered balance between reward and inhibition? Front Behav Neurosci. 2014;9(8):410.
117. BrownT, VanzhulaI, Reilly E, et al. Body mistrust bridges interoceptive awareness and eating disorder symptoms. J Abnorm Psychol. 2020;129(5):445–56.
118. Strigo I, Matthews S, Simmons A, et al. Altered insula activation during pain anticipation in individuals recovered from anorexia nervosa:
Evidence of interoceptive dysregulation. Int J Eat Disord. 2013;46:23–33.
119. Berner
L, Simmons A, Wierenga C, et al. Altered interoceptive activation before, during, and after aversive breathing load in women remitted from anorexia nervosa. Psychol Med. 2018;48(1):142–54.
120. Oberndorfer T, Simmons A, McCurdy D, et
al. Greater anterior insula activation during
anticipation of food images in women recovered from anorexia nervosa versus controls. Psychiatr Res. 2013 214 (2):132–41.
121. Bailer U, Narendran R, Frank W, et al. Amphetamine induced dopamine release increases anxiety in individuals recovered from anorexia nervosa. Int J Eat Disord. 2012;45(2):263–71.
122. Frank
G, Bailer UF, Henry S, et al. Increased
dopamine D2/D3 receptor binding after
recovery from anorexia nervosa measured by positron emission tomography and [11C]raclopride. Biol Psychiatr. 2005;58(11):908–12.
123. Wagner A, Aizenstein H, Venkatraman M, et al. Altered reward processing in women recovered from anorexia nervosa. Am J Psychiatr. 2007;164(12):1842–9.
124. Arnett J. The Oxford Handbook of Emerging Adulthood. Arnett J (Ed.). Oxford: Oxford University Press; 2015.
125. Gustavson K, Knudsen A, Nesvag R, et al. Prevalence
and stability of mental disorders among young adults: Findings from a longitudinal study.BMCPsychiatr. 2018;18(1):65.
126. US Department of Health and Human Services. National Survey of Drug Use and Health (NSDUH). www.samhsa.gov/data/ release/2019-national-survey-drug-use-and-health-nsduh-releases;
2019.
127. Twenge JM, Cooper AB, Joiner T, et al. Age, period, and cohort trends in mood disorder indicators and suicide-related outcomes in a nationally representative dataset, 2005–2017. J Abnorm Psychol. 2019;128(3):185–99.
128. Volpe U, Tortorella A, Manchia M, et al. Eating disorders: What age at onset? Psychiatr Res. 2016;30(238):225–7.
129. Mitrofan O, Petkova
H, Janssens A, et al. Care
experiences of young people with eating disorders and their parents: Qualitative study. BJPsych Open. 2019;5 (1):e6.
130. Dimitropoulos G, Landers A, Freeman V, et al. Open trial of family-based treatment of anorexia nervosa for transition age youth. J Can Acad Child
Adolesc Psychiatr. 2018;27(1):50–61.
131. Dimitroupoulos G, Freeman V, Allemang B, et al. Family-based treatment with transition age youth with anorexia nervosa: A qualitative summary of application in clinical practice. J Eat Disord. 2015;3(1):1–13.
132. Asen E, Scholz M. Multi-family Therapy: Concepts and Techniques. New York: Routledge; 2010.
133. Simic M, Eisler I. Multi-family therapy. In Loeb K, LeGrange D (Eds.),
Family Therapy for Adolescent Eating and Weight Disorders: New Applications (pp. 110–38). New York: Routledge; 2015.
134. Linehan M. DBT Skills Training Manual (2nd ed.). New
York: Guilford Press; 2015.
135. Linehan M. Dialectical
Behavior Therapy in Clinical Practice. New York: Guilford Press; 2020.
136. Zuckerman
M. Models of adult temperament. In
Handbook of Temperament (Chapter 3). New York: Guilford Press;
2012.
137. Hill L. A brain-based approach to eating disorder treatment. www.brainbasedeatingdisorders.org/; 2017.
138. Hodgekiss
A. Trying to lose weight? Try the HAND DIET: Measure food portions using just your fingers, thumbs and palm. Daily Mail; 2014.
139. Squire
L, Kandel E. Memory, from Mind to
Molecules (2nd ed.). Boulder, CO: Roberts; 2009.
140. Cross-Disorder
Group of Psychiatric Genomics
Consortium. Genomic relationships, novel loci, and pleiotropic mechanisms across eight psychiatric disorders. 2019.
141. Bulik
C, Flatt R, Abbaspour A, et al. Reconceptualizing anorexia nervosa. Psychiatr Clin
Neurosci. 2019;73 (9):518–25.
142. Liu
P, Peng G, Zhang N, et al. Crosstalk between
the gut microbiota and the brain: An update on neuroimaging findings. Front Neurol. 2019;10:833.
143. Hubel C, Yilmaz Z, Schaumberg K, et al. Body composition in anorexia nervosa: Meta-analysis and meta-regression of cross-sectional and longitudinal studies. Int J Eat Disord. 2019;52(11):1205–23.
144. AkkermannK, Paaver M, Nordquist N, et
al. Association of 5-HTT gene polymorphism, platelet MAO activity, and drive for thinness in a population-based sample of adolescent girls. International Journal of Eating Disorders. 2008;41(5):399–404.
145. Danner U, Sanders N, Smeets P, et al. Neuropsychological
weaknesses in anorexia nervosa: Set-shifting, central coherence, and decision making in currently ill and recovered women. Int J Eat Disord. 2012;45(5):685–94.
146. Frank
G, Kaye W. Current status of functional imaging in eating disorders. Int J Eat Disord. 2012;45(6):723–36.
147. Klump
K. Puberty as a critical risk period for eating disorders: A review of human and animal studies. Horm Behav. 2013;64 (2):399–410.
148. Ma R, Mikhail M, Fowler N, et al. The role of
puberty and ovarian hormones in the genetic diathesis of eating disorders in
females. Child Adolesc Psychiatr Clin N Am. 2019;28(4):617–28.
149. Simmons
W, Avery J, Barcalow J, et al. Keeping the body in mind: Insula functional organization and functional connectivity integrate interoceptive, exteroceptive, and emotional awareness. HumBrainMapp. 2013;34(11):2944–58.
150. Ehrlich
S, Lord A, Geisler D, et al. Reduced functional connectivity in the thalamo-insular subnetwork in patients with acute anorexia nervosa. Hum
Brain Mapp. 2015;36(5):1772–81.
151. Treasure J, Zipfel S, Micali N, et al. Anorexia nervosa. Nature Rev Dis Primers. 2015;1:15074.
152. Nunn
K, Frampton I, Gordon I, et al. The fault is not in her parents but in her insula – a neurobiological hypothesis of anorexia nervosa. Eur Eat Disord Rev. 2008;16 (5):355–60.
153. Nunn K, Frampton I, Lask B, et al. Anorexia nervosa and theinsula. Med Hypotheses . 2011;76(3):353–7.
154. FrankG, Shott M, Keffer C, et al. Extremes of eating are associated with reduced neural taste discrimination. Int J Eat Disord. 2016;49(6):603–12.
155. Szalavitz M. The currency of desire. Sci Am Mind.
2017;28:48–53.
156. Sullivan PF. Mortality in anorexia nervosa. Am J Psychiatr. 1995;152(7):1073–4.
157. Ackard D, Richter S, Egan A, et al. Poor outcome and death among youth, young adults, and midlife adults with eating disorders: An investigation of risk factors by age at assessment. Int J EatDisord. 2014;47(7):825–35.
158. Arcelus J, Mitchell A, Wales J, et al. Mortality rates in patients with anorexia nervosa and other eating disorders. Arch Gen Psychiatr. 2011;68(7):724–31.
159. Compan V, Walsh B, Kaye W, et al. How does the brain implement adaptive decision making to eat? JNeurosci. 2015;35(41):13868–78.
160. Brainstorm Consortium. Analysis of shared heritability in common disorders of the brain. Science. 2018;360:6395.
161. Mahon
P, Hildebrandt T, Burdick K. New genetic discoveries in anorexia nervosa: Implications for the field. Am J Pschiatr. 2017;174(9):821–2.
162. Simone
M, Askew A, Lust K, et al. Disparities in self-reported eating disorders and
academic impairment in sexual and gender minority college students relative to their heterosexual and cisgender peers. IntJ Eat Disord . 2020;53(4):513–24.
163. American
Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-V, 5th ed.). Washington, DC: American Psychiatric Association; 2013.
164. Yau
W-Y, Bischoff-Grethe A, Theilmann R,et al. Alterations in white matter microstructure in women recovered from anorexia nervosa. Int J Eat Disord. 2013;46(7):701–98.
165. Stiles-Shields C, Bamford B, Lock J, et al. The effect of driven exercise on treatment outcomes for adolescents with anorexia and bulimia nervosa.IntJ Eat Disord. 2015;48(8):392–6.
166. Zerwas S, Lund B, Von Holle A, et al. Factors associated with recovery from anorexia nervosa. J Psychiatr Pract. 2013;47(7):972–9.
167. Levinson
C, Zerwas SC, Brosof LC, et al. Associations between dimensions of anorexia nervosa and obsessive-compulsive disorder: An examination of personality and psychological factors in patients with anorexia nervosa. Eur Eat Disord Rev. 2018;27(2):161–72.
168. Klump K, Burt S, Spanos A, et al. Age differences in genetic and environmental influences on weight and shape concerns. Int J Eat Disord. 2010;43(8):679–88.
169. Klump
K, Culbert K, O’Connor S, et al. The
significant effects of puberty on the genetic
diathesis of binge eating in girls. Int J Eat Disord. 2017;50(8):984–9.
170. Hubel C, Gaspar H, Coleman J, et al. Genetic correlations of psychiatric traits with body composition and glycemic traits are sex- and age-dependent Nat Commun. 2019;10(1):5765.
171. McAdams
C, Jeon-Slaughter H, Evans S, et al. Neural differences in self-perception; Oberndorfer T, Kaye W, Simmons A, et al. Demand-specific alteration of nmedial prefrontal cortex response during an inhibition task in recovered anorexic women. Int J Eat Disord. 2011;44(1):1–8.
174. Linehan M. Cognitive-Behavioral Treatment of Borderline Personality Disorder. New York: Guilford Press; 1993.
175. Pruis T, Keel P, Janowsky J. Recovery from anorexia nervosa includes neural compensation for negative body image. Int J Eat Disord. 2012;45:919–31.
176. McCormick L, Keel P, Brumm M, et al. Implications of starvation-induced change in right dorsal anterior cingulate volume in anorexia nervosa. Int J Eat Disord. 2008;41(7):602–10.
177. Bergen
A, Yeager M, Welch R, et al. Association
of multiple DRD2 polymorphisms with anorexia nervosa. Neuropsychopharmacology. 2005;30 (9):1703–10.
178. Frieling H, Romer K, Scholz S, et al. Epigenetic dysregulation of dopaminergic genes in eating disorders. IntJ Eat Disord. 2010;43(7):577–83.
179. Richmond B, Liu Z, Shidara M. Predicting future rewards. Science. 2003;301:179–80.
180. Robinson P, Kukucska R, Guidetti G, et al. Severe and enduring anorexia nervosa (SEE-AN): A qualitative study of patients mindful eating vs. distraction during food exposure. International Journal of
Eating Disorders 2013;46(6):582–85.
185. Hill L. The wood burning stove: A metaphor for
dietary regulation for persons with eating
disorders. In Eating Disorders Treatment and Prevention, Vol. 1 (2) New York: Brunner/Mazel; 1993.
186. Kaye WH, Barbarich NC, Putnam K, Gendall KA, Fernstrom J, Fernstrom M, et al. Anxiolytic effects of acute tryptophan depletion in anorexia nervosa. Int J Eat Disord 2003;33:257–67.
187. Fairburn CG, Beglin SJ. Eating Disorder Examination Questionnaire (EDE-Q) [Database record]. APA PsycTests;1994.
188. Schebendach
J, Mayer LES, Devlin MJ, Attia E, Walsh, BT. Dietary energy density and diet variety as risk factors for relapse in anorexia nervosa: A replication. Int. J. Eat. Disord. 2012; 45:79–84. doi: 10.1002/eat.20922
189. Gianini,
LM, Walsh BT, Steinglass J, Mayer L.
Long-term weight loss maintenance in obesity: Possible insights from anorexia
nervosa? International Journal of Eating Disorders, 2017;50:341– 42. doi: 10.1002/eat.22685
190. Jewell,
T., Blessitt, E., Stewart, C., Simic, M., & Eisler, I. (2016). Family therapy for child and adolescent eating disorders: a critical
review. Family Process, 55(3), 577–594.




 ContinuingEdCourses.Net dba SocialWorkCoursesOnline.com, provider #1107, is approved as an ACE provider to offer social work continuing education by the Association of Social Work Boards (ASWB) Approved Continuing Education (ACE) program. Regulatory boards are the final authority on courses accepted for continuing education credit. ACE provider approval period: 3/9/2005-3/9/2027.
ContinuingEdCourses.Net dba SocialWorkCoursesOnline.com, provider #1107, is approved as an ACE provider to offer social work continuing education by the Association of Social Work Boards (ASWB) Approved Continuing Education (ACE) program. Regulatory boards are the final authority on courses accepted for continuing education credit. ACE provider approval period: 3/9/2005-3/9/2027. ContinuingEdCourses.Net dba SocialWorkCoursesOnline.com has been approved by NBCC as an Approved Continuing Education Provider, ACEP No. 6323. Programs that do not qualify for NBCC credit are clearly identified. ContinuingEdCourses.Net is solely responsible for all aspects of the programs.
ContinuingEdCourses.Net dba SocialWorkCoursesOnline.com has been approved by NBCC as an Approved Continuing Education Provider, ACEP No. 6323. Programs that do not qualify for NBCC credit are clearly identified. ContinuingEdCourses.Net is solely responsible for all aspects of the programs. ContinuingEdCourses.Net dba SocialWorkCoursesOnline.com is recognized by the New York State Education Department's State Board for Social Work (NYSED-SW) as an approved provider of continuing education for licensed social workers #SW-0561.
ContinuingEdCourses.Net dba SocialWorkCoursesOnline.com is recognized by the New York State Education Department's State Board for Social Work (NYSED-SW) as an approved provider of continuing education for licensed social workers #SW-0561.